
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 29(2); 2024 > Article
- Research Article
- Arterial stiffness index, physical activity and food and nutrient intake: cross-sectional study in adults aged 40 years and older
- Eun-A Kim, Yun-Mi Kim, Eun-Kyung Kim
-
Korean Journal of Community Nutrition 2024;29(2):81-96.
DOI: https://doi.org/10.5720/kjcn.2024.29.2.81
Published online: April 30, 2024
1Master’s Degree, Department of Food and Nutrition, Gangneung-Wonju National University, Gangneung, Korea 
2Graduate Student, Department of Food and Nutrition, Gangneung-Wonju National University, Gangneung, Korea
3Professor, Department of Food and Nutrition, Gangneung-Wonju National University, Gangneung, Korea
2Graduate Student, Department of Food and Nutrition, Gangneung-Wonju National University, Gangneung, Korea
3Professor, Department of Food and Nutrition, Gangneung-Wonju National University, Gangneung, Korea
-
Corresponding author:
Eun-Kyung Kim, Tel: +82-33-640-2336,
Email: ekkim@gwnu.ac.kr
Received: 16 January 2024 • Revised: 20 February 2024 • Accepted: 28 March 2024
- 193 Views
- 14 Download
- 0 Crossref
- 0 Scopus
Abstract
Objectives
This study aimed to investigate arterial stiffness index, physical activity, and food and nutrient intake in middle-aged adults over 40 years when the incidence of cardiovascular disease begins to increase.
Methods
This study included 106 subjects (48 males and 58 females) aged between 40 and 64 years. The arterial stiffness index (brachial-ankle pulse wave velocity [baPWV], and anklebrachial index [ABI]) were measured using a blood pressure pulse wave testing device. Physical activity was assessed using the Korean version of the Global Physical Activity Questionnaire, and food and nutrient intake was calculated using the Food Frequency Questionnaire.
Results
The mean age of the subjects was 54.4 years. Although the ABI of the subjects was within the normal range, they were divided into tertiles to compare physical activity and food and nutrient intake. In males, the time spent on moderate to vigorous physical activity (MVPA) was significantly higher in T3 (600.6 min/week) than in T1 (304.4 min/week). In females, the time spent in sedentary behavior was significantly lower in T3 (294.5 min/week) than in T1 (472.1 min/week). In addition, the frequency of fish consumption was significantly higher in T3 (1.27 frequency/day) than in T1 (0.64 frequency/day) in females. Polyunsaturated fatty acid (PUFA) and ω-3 fatty acid intake, adjusted for energy intake, were significantly positively correlated with ABI (r = 0.200 and r = 0.218, respectively).
Conclusions
High MVPA (in males), low sedentary behavior (in females), and PUFA and ω-3 fatty acid intake through fish consumption may be associated with low peripheral artery stiffness. Therefore, arteriosclerosis can be prevented through physical activity and proper dietary therapy.
Korean J Community Nutr. 2024 Apr;29(2):81-96. English.
Published online Apr 23, 2024.
https://doi.org/10.5720/kjcn.2024.29.2.81
Published online Apr 23, 2024.
https://doi.org/10.5720/kjcn.2024.29.2.81
© 2024 The Korean Society of Community Nutrition
Original Article
Arterial stiffness index, physical activity and food and nutrient intake: cross-sectional study in adults aged 40 years and older
Abstract
Objectives
This study aimed to investigate arterial stiffness index, physical activity, and food and nutrient intake in middle-aged adults over 40 years when the incidence of cardiovascular disease begins to increase.
Methods
This study included 106 subjects (48 males and 58 females) aged between 40 and 64 years. The arterial stiffness index (brachial-ankle pulse wave velocity [baPWV], and ankle-brachial index [ABI]) were measured using a blood pressure pulse wave testing device. Physical activity was assessed using the Korean version of the Global Physical Activity Questionnaire, and food and nutrient intake was calculated using the Food Frequency Questionnaire.
Results
The mean age of the subjects was 54.4 years. Although the ABI of the subjects was within the normal range, they were divided into tertiles to compare physical activity and food and nutrient intake. In males, the time spent on moderate to vigorous physical activity (MVPA) was significantly higher in T3 (600.6 min/week) than in T1 (304.4 min/week). In females, the time spent in sedentary behavior was significantly lower in T3 (294.5 min/week) than in T1 (472.1 min/week). In addition, the frequency of fish consumption was significantly higher in T3 (1.27 frequency/day) than in T1 (0.64 frequency/day) in females. Polyunsaturated fatty acid (PUFA) and ω-3 fatty acid intake, adjusted for energy intake, were significantly positively correlated with ABI (r = 0.200 and r = 0.218, respectively).
Conclusions
High MVPA (in males), low sedentary behavior (in females), and PUFA and ω-3 fatty acid intake through fish consumption may be associated with low peripheral artery stiffness. Therefore, arteriosclerosis can be prevented through physical activity and proper dietary therapy.
Keywords
arterial stiffness index; physical activity; food frequency questionnaire; polyunsaturated fatty acid; ω-3 fatty acid
INTRODUCTION
Cardiovascular disease (CVD), a condition affecting the heart and blood vessels, has been reported by the World Health Organization (WHO) as a major cause of death worldwide [1]. In addition, according to Korea's cause of death statistics, CVD will be the second leading cause of death in 2022, with mortality rates increasing with age [2]. According to the Statistics 2023 report, the CVD mortality rate per 100,000 people in 2022 varies by age group. The rate starts low at 6.8 in the 30s, but increases to 20.4 in the 40s, then more significantly to 46.5 in the 50s. It surpasses 100 in the 60s (104.2) and rises sharply to 2,283.5 in the 70s and older [2].
Factors that increase the risk of occurrence and death from CVDs include various health and clinical indicators such as age, sex, hypertension, diabetes, blood lipid level, family history of CVD, and smoking [3]. Particularly, the risk of asymptomatic arteriosclerosis increases as arterial stiffness increases [4, 5]. Arterial stiffness refers to a state in which the arterial wall loses its original elasticity and becomes hard due to structural and functional changes; it is used as an independent indicator to predict the risk of CVD [5, 6]. Factors closely related to associated arterial stiffness include aging, hypertension, diabetes, and dyslipidemia, as well as physical activity and dietary factors [5, 6, 7]. Among these, increased physical activity and improved diet are positive factors for preventing CVDs and improving arterial stiffness [7, 8].
Methods for measuring arterial stiffness include invasive methods such as coronary angiography and non-invasive methods such as ultrasound imaging and computed tomography. However, their clinical use is limited by high costs and surgical risks [9]. Bachial-ankle pulse wave velocity (baPWV), a non-invasive method of measuring pulse waves, was recently assessed using an oscillometric method incorporated into a blood pressure monitor cuff and paired with brachial-ankle blood pressure measurement. The ankle-brachial index (ABI) is used as an indicator of arterial stiffness [10]. baPWV refers to the speed of blood flow through the upper arm and ankle and is used to evaluate the stiffness of the arterial wall. It is known that the harder the artery, the faster the speed and the higher the risk of arteriosclerosis increases [10]. The ABI measures the blood pressure in the upper arm and ankle and is calculated by dividing the ankle systolic blood pressure by the brachial systolic blood pressure. In general, the normal level in healthy individuals is 1.0–1.4, and it has been reported that the risk of developing peripheral vascular disease increases as the level decreases to 0.9 or less [11]. On the other hand, if the ABI level is 1.4 or more, it indicates the uncompressed state due to calcification of the artery; however, this subject is excluded from the study [12].
baPWV and ABI are recognized for their high clinical utility due to several factors: simple and economical measurement methods, the ability to obtain repeatable measurements, and a growing body of research actively investigating their applications [10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23]. Therefore, studies on the relevance of physical activity, a factor affecting arteriosclerosis, have used baPWV and ABI as indicators of arterial stiffness [10, 11, 12, 13, 14, 15, 16, 17, 18].
Methods for assessing physical activity include measuring body movements using tools such as accelerometers and self-recording methods using questionnaires [10]. Because the self-recording method places a relatively low cost and burden on the subject, the Korean National Health and Nutrition Examination Survey (KNHANES) also uses the Global Physical Activity Questionnaire (GPAQ) as a physical activity evaluation tool. The GPAQ is classified into four domains: work, recreational activities, moving from place to place, and sedentary behavior; therefore, it has the advantage of being able to interpret physical activity by domain [24].
Recent studies using baPWV and ABI include the relationship between physical activity and arterial stiffness assessed with an accelerometer, an objective measurement tool in healthy adults [10]; the relationship between physical activity level assessed with an accelerometer in adult females and baPWV [12]; and the relationship between physical activity level and arterial stiffness surveyed using the GPAQ in the elderly [13].
Based on the results of previous studies [10, 13], the longer the sedentary behavior continued, the higher the risk of arteriosclerosis and peripheral arterial disease [10], and the risk of arteriosclerosis was low in the elderly who followed the WHO physical activity guidelines (moderate-intensity physical activity for a total of 150 minutes or more per week) [13]. However, since arterial stiffness is influenced not only by physical activity but also by dietary factors, it has been suggested that future research on the relationship between arterial stiffness and diet is necessary [10].
Dietary intake survey methods that can determine an individual’s food and nutrient intake include the 24-hour recall method, food recording method, and food frequency questionnaire (FFQ). Among them, the FFQ is a method for investigating the frequency of consumption over a period for the presented food items, which has the advantage of being effective in identifying long-term daily consumption trends compared with other survey methods [25]. Accordingly, it is useful for analyzing the relationship between chronic diseases and dietary factors in epidemiological research. Therefore, the FFQ is appropriate for investigating diet-related factors that affect the development of arteriosclerosis over a long period of time [26].
Kim et al. [27] compared the calculated food and nutrient intake using the FFQ and 24-hour recall in postmenopausal females, while Ha et al. [28] compared the frequency of intake of specific foods obtained from the FFQ and daily intake in adults aged 40–64 with CVD risk. However, the risk of CVD applied in these studies was the Framingham General Cardiovascular Risk Score (FRS) presented by the American Heart Association in 2008 [29], which was calculated based on sex, age, blood pressure, total cholesterol and high-density lipoprotein cholesterol in the blood, smoking status, and presence of diabetes. Iso et al. [23] also used this FRS index to track fish and ω-3 fatty acid intake and the risk of coronary artery disease in a cohort study targeting Japanese people aged 40–59 years.
Meanwhile, since arterial stiffness progresses over a long period, studies on the relationship between arterial stiffness and dietary factors [26, 30] mainly used the FFQ as a dietary survey method. Maruyama et al. [26] investigated the relationship between intake of fish and ω-3 fatty acids and carotid intima-media thickness (C-IMT) measured with ultrasound imaging equipment in adults aged 30–84 years, and Moyama et al. [30] evaluated the relationship between dietary patterns and baPWV (measured with VP-1000 Plus; Omron) in middle-aged adults.
However, it is difficult to find domestic studies that evaluate the relationship between physical activity and food and nutrient intakes by directly measuring arterial stiffness based on baPWV and ABI.
Therefore, in this study, we sought to examine arterial stiffness index, physical activity, and food and nutrient intake in middle-aged adults over 40 years in which the incidence of CVD is gradually increasing. Arterial stiffness was assessed using baPWV and ABI; physical activity was assessed using the GPAQ; and food and nutrient intake was assessed using the FFQ.
METHODS
Ethics statement
|
1. Research subject
In this study, middle-aged adults aged 40–64 years who had no difficulty in physical activities, such as walking, were recruited as research subjects through the university and local community centers in Gangneung City. A total of 113 people (51 males, 62 females) who fully understood the contents of this study and signed the consent form to participate in the study were selected as research subjects.
2. Research method
1) Anthropometrics
With the subject standing upright in light clothing, height was measured using an automatic stadiometer (BSM 330; Inbody), and body weight and body composition were measured using a body composition analyzer (InBody 620; Inbody, Seoul, Korea). Body mass index (BMI) was calculated using height and body weight.
2) Blood pressure
After resting for at least 5 minutes in a sitting position with a straight back, systolic and diastolic blood pressures were measured once using an automatic electronic blood pressure meter (HEM-7310; Omron, Seoul, Korea).
3) Arterial stiffness
Arterial stiffness was measured using a blood pressure pulse wave testing device (VP-1000 Plus; Omron, Seoul, Korea). The study subjects wore light clothing, laid in a straight position on the bed, and rested for approximately 5 minutes before the measurement. Afterward, cuffs were wrapped around both upper arms and ankles to prevent movement, and electrocardiogram (ECG) electrodes were attached to the inside of both wrists. In addition, a phonocardiogram (PCG) sensor was mounted on the left edge of the sternal area of the subject’s clothing. Measurements were taken after fixing the heart-sound sensor with a weight to prevent its movement. To reduce errors, the average value of 2 consecutive measurements was used for the analysis, and the total measurement time was approximately 10 minutes.
(1) baPWV
The baPWV was calculated using the average value of the left and right measurements of the study subjects, and the calculation formula for baPWV was as follows:
baPWV(cm/sec) = Blood Vessel Length/Pulse Wave Transmission Time Difference
The length of the blood vessels was calculated based on the subject’s height, and the difference in pulse wave transmission time was calculated using the difference in transmission time between the pulse waves measured in the limb arterial vessels.
(2) ABI
The ABI was calculated using the average value of the left and right measurements of the study subject, and the ABI calculation formula was as follows:
ABI = Ankle Systolic Blood Pressure/Brachial Systolic Blood Pressure
4) Physical activity survey
Physical activity was investigated using the Korean version of the GPAQ developed by WHO and through one-on-one interviews with the subjects by the researchers. The questionnaire focused on activities lasting at least 10 minutes in a normal week. Additionally, during one-on-one interviews, examples of activities at each level (vigorous-intensity physical activity: working at a construction site, biking, and running fast; moderate-intensity physical activity: kitchen work, cleaning, childcare, golf, yoga, weight training, and brisk walking) were provided to help the subjects understand the level of physical activity.
5) Dietary intake survey
The food and nutrient intake of the study subjects was investigated using the FFQ from the 6th KNHANES (2013–2015) and through one-on-one interviews. The survey included 112 food items and assessed dietary intake in 2 ways: frequency of consumption of each food item and the average intake per serving during the past year. The intake frequency was divided into 9 frequency intervals (almost never, once a month, 2–3 times a month, once a week, 2–4 times a week, 5–6 times a week, once a day, twice a day, and 3 times a day). As such, the average intake per serving consisted of three response options: small (0.5), medium (1.0), and large (1.5–2.0) compared to the standard amount presented in the questionnaire [31].
The subjects’ daily energy and nutrient intakes were calculated by referring to the calculation method in the Food Intake Frequency Survey Nutrient Ingredients DB User Guide. The frequency of intake over the past year was calculated as the daily intake frequency of the corresponding food using a median of nine frequency intervals.
In addition, the one-time intake was converted by calculating the ratio based on the standard amount of each item in the questionnaire. The daily energy and nutrient intake for each food item were calculated based on the daily intake frequency and the intake ratio compared to the standard amount using the following formula:
Daily Energy and Nutrient Intake by Food Item = Daily Intake Frequency × Intake Ratio per Standard Serving × Nutrient Content
To calculate the frequency of daily intake by food group, 112 food items in the survey were categorized into 19 groups according to the data analysis criteria suggested by the KHNANES [31].
6) Medical history, menopause, and smoking status survey
History of hypertension, diabetes, and dyslipidemia, which are major risk factors for CVD, as well as the intake of medications for the diseases, menopausal status, and smoking status were investigated through a self-administered questionnaire or through a one-on-one interview.
3. Statistical analysis
All data collected in this study was statistically processed and analyzed using IBM SPSS statistics 28.0 (IBM Corporation, Armonk, NY, USA). Among the 113 recruited research subjects, seven people were excluded due to insufficient answers to the questionnaire using the FFQ. Finally, the data of the remaining 106 people (48 males, 58 females) were used for analysis.
The Kolmogorov-Smirnov test was used to assess the normality of the collected variables; the results showed that the variables were not normally distributed, therefore, a nonparametric test was performed for further analysis. In addition, all investigated values are expressed as mean and standard deviation. The Mann-Whitney U test was used to compare the study subjects’ anthropometric measurements, blood pressure, arterial stiffness index, and time spent on physical activity between the sexes.
Since the ABI measurement values of the subjects were within the normal range of 1.0–1.4, comparison with subjects outside the normal range (e.g. ABI < 1.0) was difficult. Accordingly, the subject’s ABI value was divided into tertiles, with the lower group being T1 (< 1.08), the middle group being T2 (1.08 ≤ T2 < 1.18), and the upper group being T3 (≥ 1.18). The Mann-Whitney U test was used to compare the subjects’ physical activity time and frequency of intake by food group (T1 and T3). The significance of sex distributions for age groups (40–49, 50–59, and 60–64), BMI (< 25.0 kg/m2 and ≥ 25.0 kg/m2), and smoking status (current, past, and never) was assessed using the χ2 test. In addition, an analysis of covariance adjusted for sex was performed to compare blood pressure and arterial stiffness index by age group. To analyze the relationship among arterial stiffness index, physical activity, and nutrient intake, a partial correlation analysis was performed after adjusting for age, sex, BMI, medical history (hypertension, diabetes, and dyslipidemia), and menopause. A two-side test was conducted on all the data, and significance was tested at a significance level of 5%.
RESULTS
1. General characteristics
Table 1 shows the anthropometric measurements, distribution of age and BMI, smoking status, medical history, and menopausal status of the participants in this study. The average age was 53.3 and 55.2 years for males and females, respectively, showing no significant difference by sex. Height and body weight were significantly higher for males (170.4 cm, 71.8 kg) than for females (157.8 cm, 58.1 kg) (P < 0.001). BMI calculated based on height and body weight was also significantly higher for males (24.8 kg/m2) than for females (23.3 kg/m2) (P < 0.01), while body fat percentage was significantly lower in males (23.6%) than in females (31.9%) (P < 0.001).
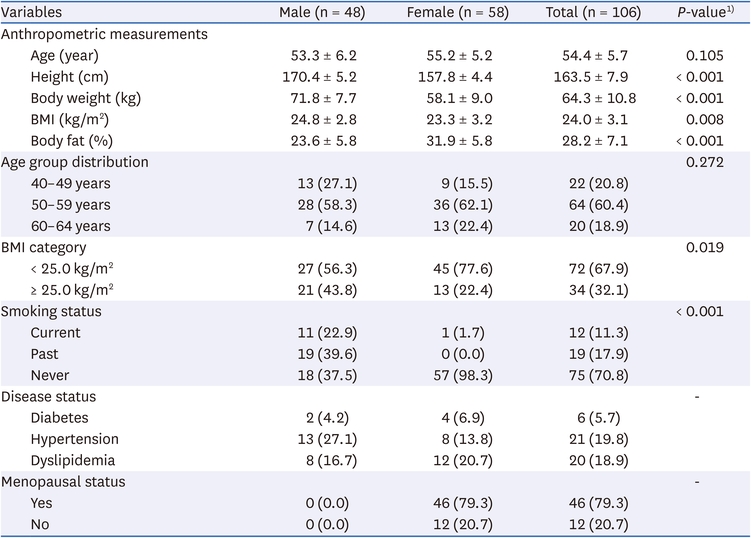
Table 1
General characteristics of the subjects by sex
Looking at the obesity rate evaluated according to the Korean Society for Obesity Treatment Guidelines (2020), the proportion of males and females with a BMI of 25 kg/m2 or higher was 43.8% and 22.4%, respectively, showing significantly different distributions between sexes. The survey of smoking status revealed that among males, 11 (22.9%) were current smokers, 19 (39.6%) were past smokers, and 18 (37.5%) were non-smokers; in females, one (1.7%) was a current smoker, and the remaining 57 (98.3%) were non-smokers.
From the assessment of medical history, 6 (5.7%) had diabetes, 21 (19.8%) had hypertension, and 20 (18.9%) had dyslipidemia. Additionally, among the female subjects, 46 (79.3%) were postmenopausal.
2. Blood pressure and arterial stiffness index by sex and age group
All study subjects were classified based on sex and age, and blood pressure and arterial stiffness index were compared between each group (Table 2). When comparing the study subjects by sex, both systolic and diastolic blood pressures showed no significant differences. Additionally, the baPWV, an indicator of arterial stiffness, was 1,322.2 and 1,325.8 cm/sec for males and females, respectively, showing no significant difference between sexes. In contrast, the ankle-brachial index (ABI), which can predict the stiffness of peripheral blood vessels, was significantly lower in females (1.11) than in males (1.16) (P < 0.001).

Table 2
Blood pressure and arterial stiffness index of the subjects by sex and age group
When all study subjects were divided by age groups of 40–49, 50–59, and 60–64 years old, the proportion of females was 40.9%, 56.3%, and 65.0%, respectively. There was no significant difference. Blood pressure did not show any significant difference between age groups in both systolic and diastolic periods, while baPWV was significantly higher in those aged 60–64 years (1,412.0 cm/sec) compared to those aged 40–49 years (1,265.6 cm/sec). In contrast, the ABI was significantly lower in those aged 40–49 years (1.09) than in those aged 50–59 years (1.14) and 60–64 years (1.16) groups.
3. Physical activity surveyed by the GPAQ
Table 3 shows the time spent by domain and the intensity of the physical activity surveyed using the GPAQ. There was no significant difference by sex in the time spent on vigorous-intensity physical activity among activities in the work domain. However, the time spent on moderate-intensity physical activity was significantly higher for females (510.2 min/week) than for males (297.1 min/week) (P < 0.001). On the other hand, the time spent on vigorous-intensity physical activity among recreational activities was significantly higher for males (115.0 min/week) than for females (31.0 min/week) (P < 0.001). There was no significant difference in time spent on moderate-intensity physical activity by sex. Meanwhile, the time spent on sedentary behavior was significantly higher in males (562.5 min/day) than in females (446.0 min/day) (P < 0.01).
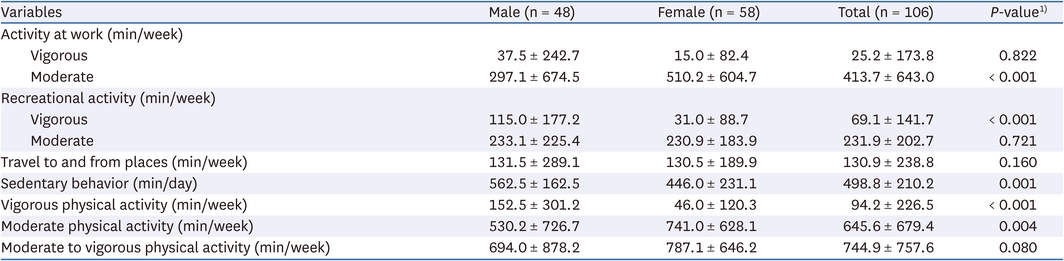
Table 3
Time spent on physical activity by domain and intensity using GPAQ by sex
The time spent on vigorous-intensity physical activity was significantly higher in males (152.5 min/week) than in females (46.0 min/week) (P < 0.001), but the time spent on moderate-intensity physical activity was significantly higher in females (741.0 min/week) than in males (530.2 min/week) (P < 0.01). Meanwhile, the sum of time spent on moderate-intensity and vigorous-intensity physical activity in all domains (moderate to vigorous physical activity, MVPA) was 787.1 and 744.9 min/week, respectively, showing no significant difference by sex.
4. Time spent on physical activity by domain and intensity by ABI
Although all participants in this study had ABI within the normal range, we investigated whether physical activity levels differed even among these individuals. To do this, we divided the ABI values into tertiles based on ABI values and compared physical activity across these groups (Table 4).
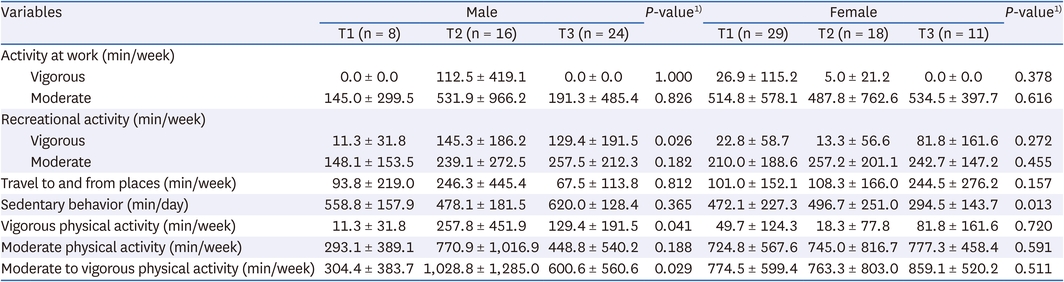
Table 4
Time spent on physical activity by domain and intensity by ABI
For males, the time spent on recreational vigorous-intensity physical activity was significantly lower in T1 (11.3 min/week) than in T3 (129.4 min/week) (P < 0.05); excluding this, there was no significant difference in the time spent on physical activity by domain and intensity. For females, the time spent on sedentary behavior was significantly higher at T1 (472.1 min/day) than at T3 (294.5 min/day) (P < 0.05); however, there was no significant difference in the time spent on physical activities.
For males, the time spent on vigorous-intensity physical activity per week was significantly higher in T3 (129.4 min/week) than in T1 (11.3 min/week) (P < 0.05); the sum of time spent on moderate-intensity and vigorous physical activities was also significantly higher in T3 (600.6 min/week) than in T1 (304.4 min/week) (P < 0.05). However, for females, there was no significant difference in the time spent on physical activity by activity intensity according to the ABI.
5. Daily frequency of food group intake by ABI
To determine whether there was a difference in the daily frequency of intake by food group depending on whether the ABI within the normal range was high or low, the ABI was divided into tertiles and compared among the 3 groups (Table 5).
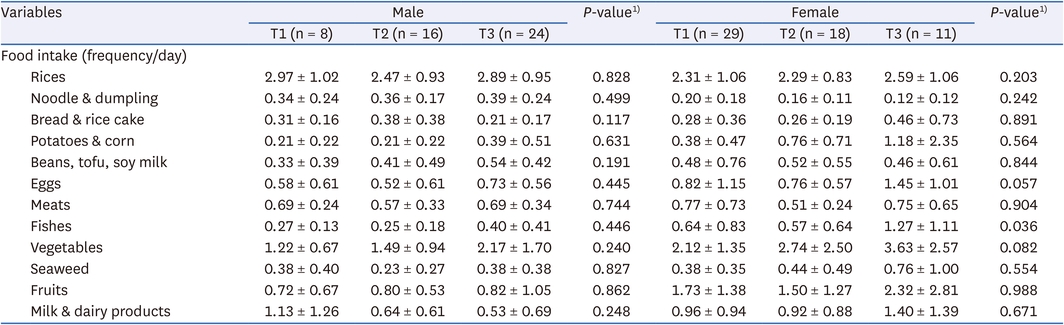
Table 5
Daily frequency of food group intake by ABI
As a result, males showed no significant difference between T1 and T3, while females’ frequency of fish consumption was significantly higher in T3 (1.27 frequency/day) than in T1 (0.64 frequency/day) (P < 0.05).
6. Relationship between physical activity and nutrient intake and arterial stiffness index
After adjusting for age, sex, BMI, medical history, and menopausal status, which are known to be related to arterial stiffness, the partial correlations between arterial stiffness index (baPWV and ABI), physical activity, and nutrient intake per 1,000 kcal are shown in Table 6. baPWV did not show a significant relationship with physical activity-related indicators and nutrient intake.
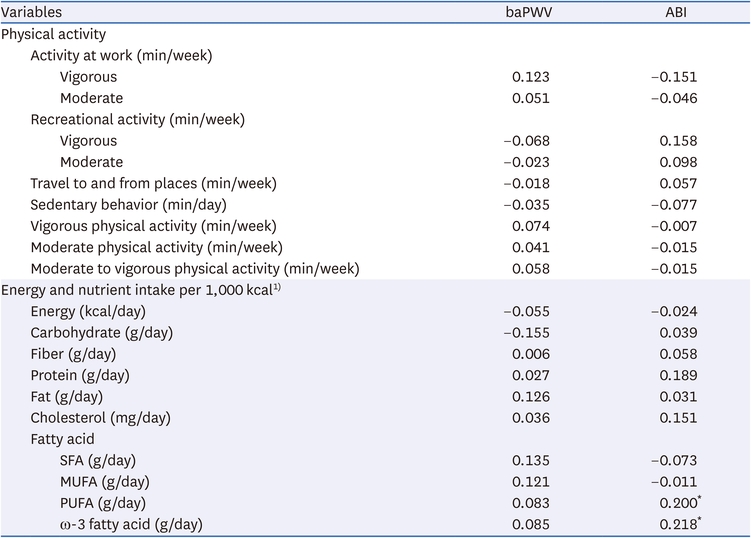
Table 6
Correlation of physical activity, nutrient intake and arterial stiffness index
However, the ABI showed a significant positive correlation of r = 0.200 and r = 0.218 with polyunsaturated fatty acids (PUFA) and ω-3 fatty acids, respectively, among nutrient intakes adjusted for energy intake (P < 0.05).
DISCUSSION
In this study, we examined arterial stiffness index, physical activity, and food and nutrient intake in middle-aged adults over 40 years—a demographic group with a rising incidence of CVD. Arterial stiffness was assessed using PWV and ABI, physical activity was assessed using the GPAQ, and food and nutrient intake was assessed using the FFQ.
The average age of the subjects of this study was 53.3 and 55.2 years for males and females, respectively, and their average height and body weight were similar to the average height and body weight of adults in the Gangwon region reported in the 2021 Health Checkup Statistical Yearbook [32]. This study’s obesity rates, determined using a BMI cut-off of 25 kg/m2, were 43.8% for males and 22.4% for females. These values are similar to the national obesity rates reported in the 2021 Statistical Yearbook of Health Examination (48.8% for males and 29.4% for females), which employed the same BMI criteria. The smoking rate of the subjects in this study (males, 22.9%; females, 1.7%) was lower than what was reported in the 2021 KNHANES (males, 31.3%; females, 7.1%) [33].
The blood pressure and arterial stiffness index of the subjects (Table 2) did not show any significant differences by sex or age group. The baPWV (male, 1,332.2 cm/sec; female, 1,325.8 cm/sec) obtained by this study was similar to the baPWV (male, 1,302.2 cm/sec; female, 1,259.7 cm/sec) of Korean adult males and females aged 20–64 years (average age 47.7 years), with no significant difference between sexes as reported by Lee et al. [10].
Meanwhile, our analysis of baPWV by age group revealed a significant difference. The group aged 60–64 years (1,412.0 cm/sec) had a higher baPWV compared to the group aged 40–49 years (1,265.6 cm/sec). This shows a significant difference between age and baPWV (r = 0.278, P < 0.01), showing that the baPWV also increased with age (the correlation between the basic characteristics of the study subjects, such as age, height, body weight, and BMI, and the arterial stiffness index is not shown in the table). Tomiyama et al. [19] also reported that baPWV significantly increased with age in Japanese people aged 25–87 years, and Ishida et al. [12] also reported that there was a significant positive correlation between baPWV and age in Japanese people aged 21–89 years. These findings suggest that arterial wall tissue changes and decreased elasticity as individuals age [6].
In this study, the ABI (1.16 for males, 1.11 for females) obtained were similar to those of American adults (1.13 for males, 1.09 for females; average age 57.0 years) reported by Kapoor et al. [20] and was significantly lower in females than in males. In a study by Ishida et al. [12], which evaluated the relationship between ABI, age, and sex, the ABI of females was found to be lower than that of males, similar to this study. These results may be related to the high proportion of postmenopausal females (79.3%) among the female subjects in this study. In other words, it has been reported that a decrease in the secretion of estrogen, a female hormone, after menopause affects the development of CVDs such as arteriosclerosis [34]. In addition, a study by Li et al. [35] also reported an increased risk of developing arteriosclerosis in postmenopausal females. Based on these previous studies [12, 20, 34, 35], ABI is associated with age, sex and menopause.
When ABI was compared by age group in this study, those aged 40–49 years had significantly lower ABI than those aged 50–59 and 60–64 years. About this, a study by Matt et al. [21] observed increasing ABI with age in Americans aged 27–95 years, showing that ABI also increased with age in subjects aged 70 years or younger. Since the stiffness of arteries due to aging increases more rapidly in central arteries than in peripheral blood vessels, it has been reported that the increase in systolic blood pressure in the upper arm is greater than in the systolic blood pressure in the ankle [36]. These results were also found to affect the ABI, which is the ratio of the ankle to brachial systolic blood pressure.
Using the GPAQ to examine physical activity levels (Table 3), we found that the time spent on moderate-intensity physical activity in the work domain, which includes household tasks such as cleaning, kitchen work, and childcare, was significantly higher for females, at about 8.5 hours per week (510.2 min/week), compared to about 5 hours per week (297.1 min/week) for males. A possible explanation for this observation is the gender disparity in housework and childcare participation, with females typically taking on a larger share of these responsibilities.
On the other hand, the time spent on vigorous recreational physical activities, including climbing, swimming, and badminton, was significantly higher for males at about 2 hours per week (115.0 min/week) compared to females at about 30 minutes per week (31.0 min/week). This is related to the fact that in the one-on-one interviews conducted with the GPAQ for this study, 24 (50.0%) of all male subjects engaged in vigorous physical activities such as biking and swimming for more than 1 hour.
Meanwhile, males spent about 9 hours and 22 minutes (562.5 min/day) per day in sedentary behavior, which was significantly higher than females who spent about 7 hours and 26 minutes (446.0 min/day). Looking at the time spent on sedentary behavior reported by Lim et al. [37], who analyzed data from the 2014–2015 KNHANES and evaluated the physical activities of Koreans (19–64 years old) using an accelerometer, males spent approximately 8 hours and 22 minutes (502.9 minutes/day for males), and females spent approximately 8 hours and 18 minutes (498.9 minutes/day for females). In this study, males spent approximately 1 more hour and females spent approximately 53 minutes less. This is believed to be related to differences in the subjects or measurement tools used in each study. In general, physical activity questionnaires such as the GPAQ are subjective measurement methods that rely on the memory of the respondents and may have lower accuracy than an accelerometer, which is an objective measurement tool [38].
The GPAQ used in this study to investigate physical activity does not assess the time allotment and intensity of all physical activities within 24 hours, which can be done with physical activity diaries; instead, the questionnaire assesses the time allotment by activity intensity (moderate and vigorous) according to the domain of physical activity (work, recreational activities, moving from place to place, and sedentary behavior) for a week. Therefore, to predict the subject’s overall physical activity level, the sum of the time spent on moderate to vigorous physical activity in all domains (MVPA) is presented.
Ishida et al. [12] found that out of 91,962 people who participated in the daily health examination program organized by the Okinawa General Health Maintenance Association from 2003 to 2010, only 13,211 people (51.4 years for males and 52.8 years for females) voluntarily participated in the ABI measurement and only 67 people had an ABI of less than 0.5%. Therefore, to better understand the relationship between the arterial stiffness index (ABI) and related factors, further research is needed. This could involve large-scale studies similar to those described earlier or utilizing existing data from national surveys like the National Health and Nutrition Examination Survey (NHANES) as in Kulinski et al. [17]. Additionally, studies should aim to include patients with low-grade peripheral vascular disease. However, since this study was conducted on mostly healthy adults (106 people) in addition to some patients with diabetes, hypertension, and dyslipidemia, all subjects showed ABI values in the normal range (1.0–1.4).
In the case of physical activity, the time spent on vigorous leisure-time activity in males was significantly higher in the upper ABI group at T3 (129.4 min/week) than in the lower ABI group at T1 (11.3 min/week). Wilson et al. [15] surveyed American adults aged 40 years or older and found that the prevalence of peripheral artery disease significantly decreased in the group that spent more time engaging in recreational activities. In addition, a study by Heikkilä et al. [16] in Finland investigated adults (average age 59.0 years) with borderline ABI levels (0.90–1.00) who had undergone CVD procedures. Interestingly, the group with high ABI was found to engage in a significant amount of leisure-time activities. These results suggest that physical activities, such as recreational activities, can reduce the risk of developing CVD.
Meanwhile, the time spent on sedentary behavior by females was significantly higher at T1 (472.1 min/week) than at T3 (294.5 min/week). In a study by Kulinski et al. [17], who investigated the time spent on sedentary behavior among American adults (average age 61.0 years) using accelerometers, the ABI (1.05) of the group spending approximately 10.2 hours per day on sedentary behavior was 1.05. This was significantly lower than the ABI (1.08) of the group that spent approximately 6 hours. Additionally, in a study by Lee et al. [10] targeting Korean adults aged 20–64 years, a negative correlation was found between the ABI and sedentary behavior. These results show that the longer the time spent in sedentary behavior, the higher the risk of developing peripheral artery disease.
In terms of daily intake frequency by food group, there was no significant difference between T1, T2, and T3 in males, whereas in females, the fish intake frequency of T3 (1.27 frequency/day) was significantly higher than that of T1 (0.64 frequency/day). In this regard, a study by Frank et al. [22] on female nurses (34–59 years old) in the United States showed that the risk of CVD decreased as the frequency of consumption of fish and ω-3 fatty acids increased. Additionally, a Japanese (40–59 years old) cohort study by Iso et al. [23] found that fish consumption more than once per week reduced the risk of heart disease.
There was no significant correlation between arterial stiffness index and physical activity (Table 6). In a study by Lee et al. [10], no significant correlation was found between physical activity-related indicators assessed using an accelerometer and arterial stiffness index in healthy adults. On the other hand, a study by Hawkins et al. [18], which evaluated the relationship between physical activity and ABI in Americans aged 40 years or older, found that the group of subjects with an ABI level of 0.9 or less spent less time on physical activity. These results are thought to be related to the fact that among the study subjects of Hawkins et al. [18], 98 (17.5%) had an ABI of less than 1.0, whereas this study had no comparable subjects.
Meanwhile, in this study, a significant positive correlation was found between the intake of PUFAs and ω-3 fatty acids adjusted for energy intake and ABI (Table 6). This is supported by the study of Zanetti et al. [39], which reported that ω-3 fatty acids can have a beneficial effect on reducing arterial wall stiffness and the occurrence of CVDs. In addition, a study by Maruyama et al. [26] on Japanese people (30–84 years old) also showed a significant negative correlation between ω-3 fatty acid intake and C-IMT.
This study has several limitations. First, because this study was conducted in a small number of people, most of whom were healthy, all subjects had ABI values within the normal range. Accordingly, a major limitation is that even for subjects within the normal ABI range, their ABI values could be divided into tertiles to examine how related factors differ depending on high and low ABI. Second, it is difficult to determine the relationship between exposure factors and disease, as this was a cross-sectional study that simultaneously investigated exposure and outcome factors. Third, considering that arteriosclerosis progresses over a long period, there may be limitations in evaluating the relationship with arterial stiffness using only the amount of physical activity during a week, that is, a short period of physical activity. In addition, the physical activity questionnaire (GPAQ) used in this study may have limitations in terms of accuracy and reliability, because it relies on the memory of respondents.
Nevertheless, this study is meaningful in that it directly measured baPWV, which represents central artery stiffness, and ABI, which represents peripheral vascular stiffness, in middle-aged adults over 40 years, considering that most studies that have evaluated cardiovascular risk in Korea used the Framingham General Cardiovascular Risk Center (FRS) suggested by the American Heart Association [29] in 2008. In addition, food and nutrient intakes were investigated using the FFQ, which can identify long-term daily intake patterns, as well as physical activity, using the GPAQ. This study observed that males in the high ABI group (T3), which had relatively low peripheral artery stiffness, spent more time on vigorous leisure activities such as biking, swimming, and badminton compared to the low ABI group (T1), while females in the high ABI group (T3) spent less time on sedentary behavior compared to the low ABI group (T1). Additionally, the intake of fish, PUFA, and ω-3 fatty acids showed a significant positive correlation with ABI.
CONCLUSIONS
In this study, we examined arterial stiffness index, physical activity, and food and nutrient intake in middle-aged adults over 40 years in which the incidence of CVD is gradually increasing. In Korea, surveys using accelerometers and arterial stiffness index have been conducted by the Rural Development Administration. Accordingly, in the future, research results on the factors affecting arterial stiffness should be reported through large-scale epidemiological studies at the national level, as in other countries. In addition, follow-up studies should be conducted to measure arterial stiffness in middle-aged and elderly people with a high mortality rate from CVD and analyze the relationship between food and nutrient intake, along with evaluating physical activity using objective physical activity measurement tools such as accelerometers. Based on these results, we hope to establish a detailed dietary and physical activity guideline to prevent arteriosclerosis in Koreans.
Notes
Conflict of Interest:There are no financial or other issues that might lead to conflict of interest.
Funding:This research was supported by a grant from Gangneung-Wonju National University.
Data Availability:The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
References
-
World Health Organization (WHO). The top of 10 causes of death [Internet]. WHO; 2020 [updated 2020 Dec 9]. [cited 2023 Sep 5].Available from: https://www.who.int/news-
room/fact- sheets/detail/the- top- 10- causes- of- death.
-
-
Statistics Korea. Causes of death statistics 2022 [Internet]. Statistics Korea; 2023 [updated 2023 Sep 21]. [cited 2023 Oct 26].
-
-
O’Donnell CJ, Elosua R. Cardiovascular risk factors. Insights from Framingham Heart Study. Rev Esp Cardiol 2008;61(3):299–310.
-
-
Jang HJ, Koh HM, Jang JY, Lee HJ, Moon JS, Ji JM, et al. Relationship between body composition and arterial stiffness in Korean adults. Korean J Fam Pract 2023;13(1):23–30.
-
-
Son JS, Lee RD, Hwang MH. Effects of resistance training intensity on arterial stiffness in healthy adults. Exercise Science 2023;32(3):233–241.
-
-
Lee NB, Im JJ, Park YB, Jeon YJ. Development of a pulse wave velocity measurement system and assessment of the system reproducibility for the diagnosis of arteriosclerosis. J Soc Korean Med Diagn 2005;9(1):112–124.
-
-
Lee H, Park KW, Jun HY, Gwak JY, Kim EK. Association between physical activity measured using an accelerometer and arterial stiffness based on pulse wave velocity and ankle-brachial index in healthy adults. J Nutr Health 2022;55(4):506–520.
-
-
Lee RD, Kang YJ, Hwang MH. The relationship between physical activity level and arterial stiffness in young female adults. Exercise Science 2019;28(3):232–239.
-
-
Lee HJ, Gwak JY, Jun HY, Kim EK. Relationship between arterial stiffness and physical activity level assessed by Global physical activity questionnaire (GPAQ) in the elderly. Korean J Community Nutr 2020;25(3):236–245.
-
-
Heikkilä A, Venermo M, Kautiainen H, Aarnio P, Korhonen P. Physical activity improves borderline ankle-brachial index values in a cardiovascular risk population. Ann Vasc Surg 2016;32:50–56.
-
-
Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). Z Gesundh wiss 2006;14(2):66–70.
-
-
Kim HB, Kim HS, Kwon OR, Park HJ. Food and nutrient intake level by the risk of osteoporosis and cardiovascular disease in postmenopausal women: the use of the 5th korean national health and nutrition examination surveys (2010–2011). Korean J Community Nutr 2019;24(2):152–162.
-
-
Ha AW, Kim WK, Kim SH. Intakes of milk and soymilk and cardiovascular disease risk in Korean adults: a study based on the 2012~2016 Korea National Health and Nutrition Examination Survey. J Korean Soc Food Sci Nutr 2023;52(5):522–530.
-
-
D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 2008;117(6):743–753.
-
-
Moyama S, Minami K, Yano M, Okumura M, Hayashi S, Takayama H, et al. Relationship between dietary patterns and brachial-ankle pulse wave velocity among middle-aged adults in Japan. Asia Pac J Clin Nutr 2017;26(3):539–544.
-
-
Yun SH, Shim JS, Kweon SH, Oh KW. Development of a food frequency questionnaire for the Korea National Health and Nutrition Examination Survey: data from the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Korean J Nutr 2013;46(2):186–196.
-
-
National Health Insurance Service. 2021 National Health Screening Statistical Yearbook. Wonju: National Health Insurance Service; 2022. pp. 50-787.
-
-
Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. Korea Health Statistics 2021: Korea National Health and Nutrition Examination Survey (KNHANES VIII-3). Cheongju: Korea Disease Control and Prevention Agency; 2022. pp. 3-344.
-
-
Lim JJ, Sung HY, Lee O, Kim YS. Physical activity in south Korea measured by accelerometer: the Korea National Health and Nutrition Examination Survey VI 2014-2015. Korean J Sport Sci 2020;31(2):169–179.
-
 Cite
Cite

