
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 31(2); 2026 > Article
-
Review
- The transition of nutritional status in infants, young children, and school-aged children in Korea and future-oriented nutritional strategies: a narrative review
-
Yoonna Lee†

-
Korean Journal of Community Nutrition 2026;31(2):115-126.
DOI: https://doi.org/10.5720/kjcn.2026.00115
Published online: April 30, 2026
Associate Professor, Department of Food and Nutrition, Shingu College, Seongnam, Korea
- †Corresponding author: Yoonna Lee Department of Food and Nutrition, Shingu College, 377 Gwangmyeong-ro, Jungwon-gu, Seongnam 13174, Korea Tel: +82-31-740-1528 Fax: +82-31-740-1590 Email: ynlee@shingu.ac.kr
• Received: March 18, 2026 • Revised: April 12, 2026 • Accepted: April 15, 2026
© 2026 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 770 Views
- 31 Download
- Abstract
- INTRODUCTION
- METHODS
- SECULAR TRENDS IN PHYSICAL GROWTH AND NUTRITIONAL STATUS AMONG KOREAN INFANTS AND SCHOOL-AGED CHILDREN
- ACHIEVEMENTS AND CHALLENGES OF MAJOR DOMESTIC NUTRITION POLICIES
- GLOBAL PARADIGM SHIFT IN NUTRITION STRATEGY AND FUTURE DIRECTIONS FOR INFANT AND SCHOOL-AGE NUTRITION POLICY IN KOREA
- CONCLUSIONS
- NOTES
- REFERENCES
Abstract
-
Objectives
- This study examined the secular trends in anthropometric changes and the nutritional transition among Korean infants and school-aged children, while evaluating the efficacy and constraints of existing state-led nutritional policies. Ultimately, it proposes a “systems-centered” nutrition strategy, aligned with the United Nations Children’s Fund (UNICEF) Nutrition Strategy 2020–2030, to ensure health equity for future generations.
-
Methods
- We reexamined comprehensive national health statistics, including school health examination data (1965–2024) and the Korea National Health and Nutrition Examination Survey (1998–2023). Additionally, Dietary Screening Test results from 126,768 young children (2021–2024) were reviewed. These quantitative findings were synthesized through a narrative review of South Korean pediatric nutrition policies and UNICEF’s global strategic frameworks.
-
Results
- While Korean children have historically experienced rapid secular growth, this has decelerated in the 2000s. Conversely, the prevalence of obesity has surged along with stagnant underweight rates. Dietary problems such as insufficient vegetable intake and frequent consumption of sweet snacks were also found, accelerating the “triple burden” of malnutrition. Policies such as school lunches, NutriPlus program, and Center for Children’s Foodservice Management have demonstrated great success in reducing nutritional risks and improving dietary habits. However, existing fragmented programs face limitations in comprehensively addressing regional disparities or blind spots and in providing tailored nutritional management. Conclusion: A paradigm shift is imperative to fundamentally resolve these multidimensional nutritional crises. Moving beyond fragmented programs, we need to adopt a “systems-centered” approach integrating health, education, and welfare ecosystems. Key policy recommendations include establishing a continuous life-cycle health database, introducing artificial intelligence and FoodTech-driven precision nutrition coaching, and fostering a healthy food environment through public-private partnerships within a community integrated care network.
INTRODUCTION
METHODS
SECULAR TRENDS IN PHYSICAL GROWTH AND NUTRITIONAL STATUS AMONG KOREAN INFANTS AND SCHOOL-AGED CHILDREN
ACHIEVEMENTS AND CHALLENGES OF MAJOR DOMESTIC NUTRITION POLICIES
GLOBAL PARADIGM SHIFT IN NUTRITION STRATEGY AND FUTURE DIRECTIONS FOR INFANT AND SCHOOL-AGE NUTRITION POLICY IN KOREA
CONCLUSIONS
-
CONFLICT OF INTEREST
There are no financial or other issues that might lead to conflict of interest.
-
FUNDING
None.
-
ACKNOWLEDGEMENTS
This study was based on a presentation delivered at the 2025 Fall Conference of the Korean Society of Community Nutrition.
-
DATA AVAILABILITY
The data that support the findings of this study are openly available in “School Health Information Center” at https://www.schoolhealth.kr/web/srs/selectPublicDataList.do and in “KNHANES” at https://knhanes.kdca.go.kr/knhanes/archive/wsiStatsClct.do.
NOTES
Fig. 1.Secular trends in the height of Korean children. (A, C) Anthropometric survey data by the Korean Pediatric Society and the Ministry of Health and Welfare [3,4]. (B, D) National school health examination data by the Ministry of Education [5-9].
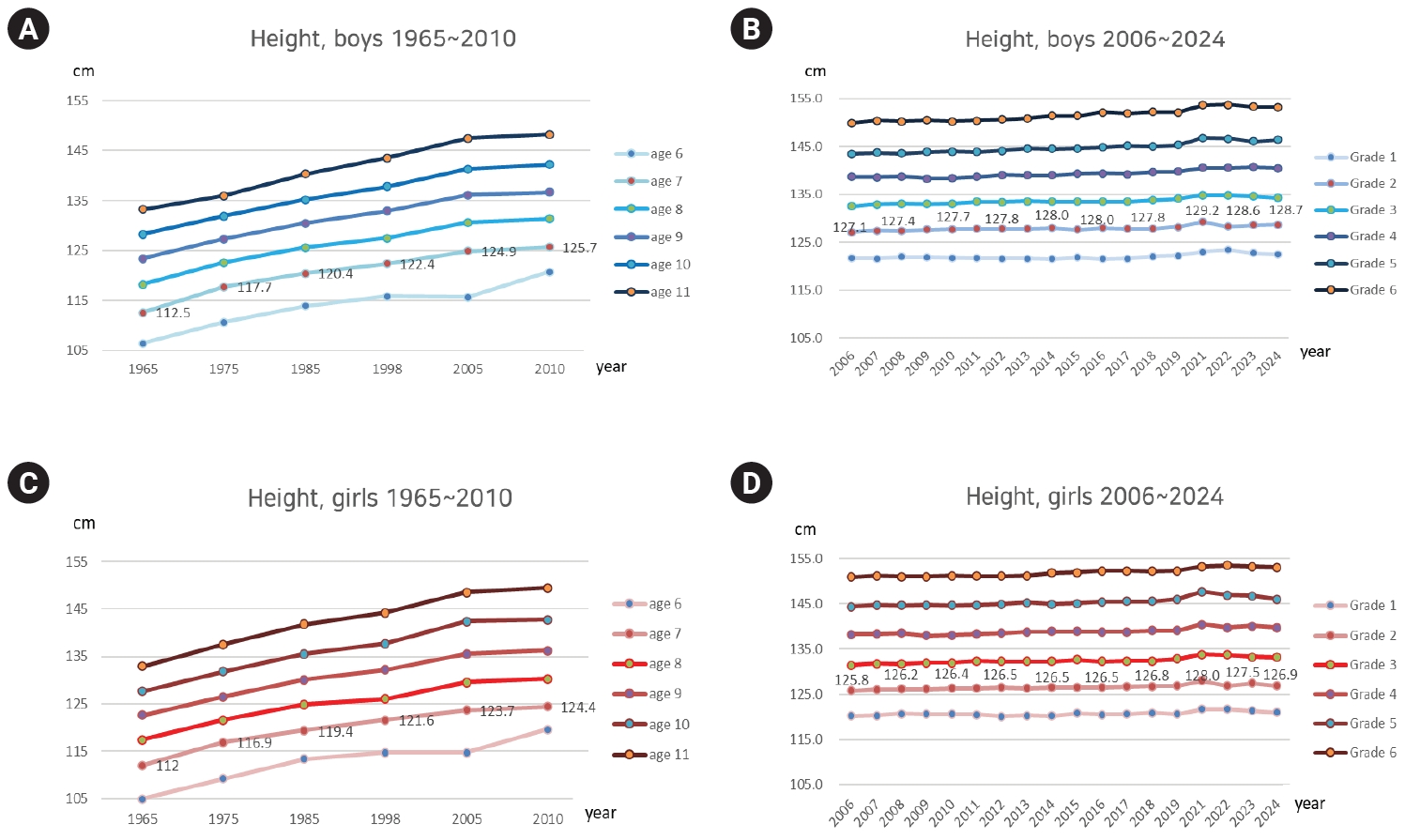
Fig. 2.Long-term trends in the prevalence of obesity and underweight among Korean elementary school children. (A) Prevalence of obesity (BMI ≥ 95th percentile) (data by the Ministry of Education) [5-9]. (B) Prevalence of underweight (BMI < 5th percentile) (data by the Ministry of Education) [5-9]. BMI, body mass index.
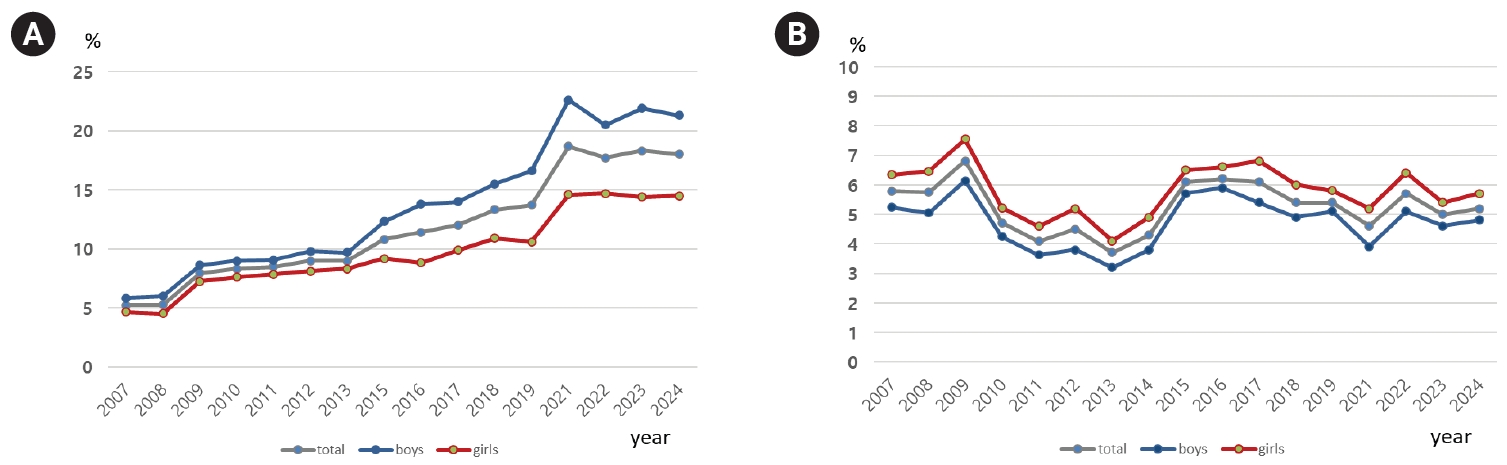
Fig. 3.Long-term trends in the prevalence of inadequate nutrient and vegetable intake in Korean children. (A) Prevalence of inadequate nutrient intake: the proportion of the population whose energy intake is less than 75% of the estimated energy requirement and whose intake of calcium, iron, vitamin A, and riboflavin is less than the estimated average requirement, as reported in Korea Health Statistics 2023 [15]. (B) Vegetable intake as reported in Korea Health Statistics 2023 [15].
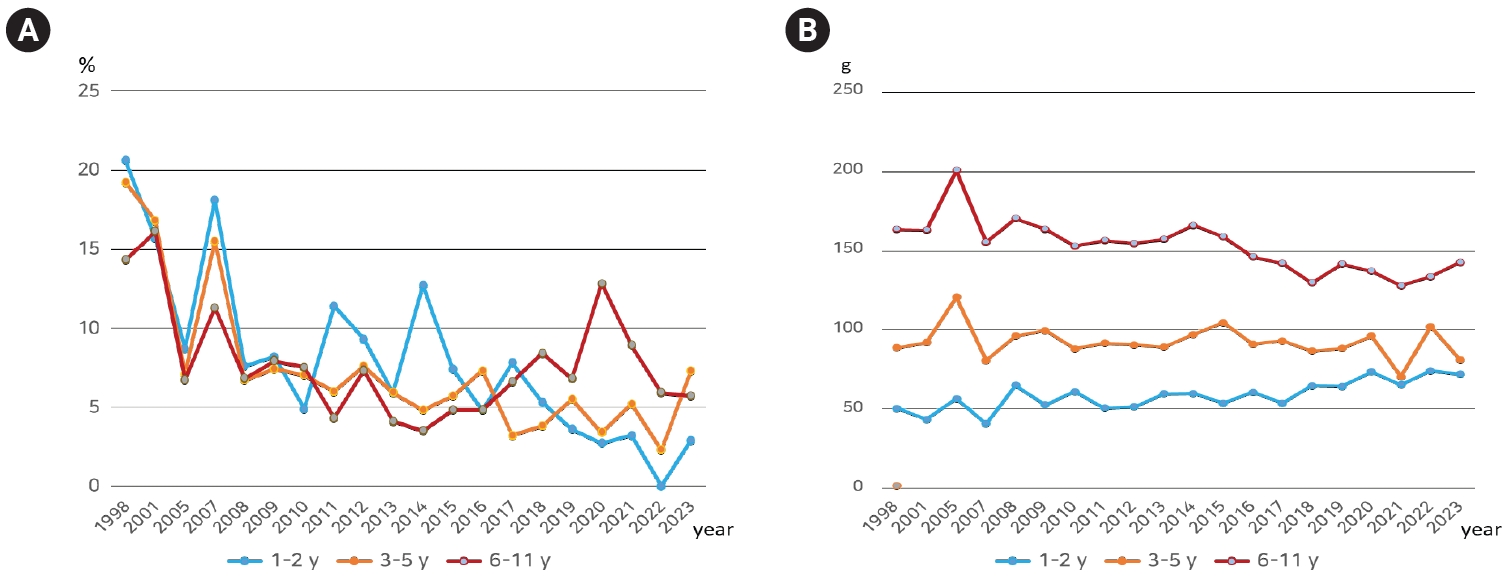
Table 1.Historical overview of nutrition policies for school-aged children and infants/young children in Korea
- 1. United Nations Children’s Fund (UNICEF). The state of the world’s children 2019: children, food and nutrition: growing well in a changing world. UNICEF; 2019.
- 2. United Nations Children’s Fund (UNICEF). Nutrition, for every child: UNICEF nutrition strategy 2020–2030. UNICEF; 2020.
- 3. Lee CG. Anthropometric changes in Korean children and adolescents. J Korean Med Assoc 2008; 51(12): 1068-1071. Article
- 4. Moon JS. Secular trends of body sizes in Korean children and adolescents: from 1965 to 2010. Korean J Pediatr 2011; 54(11): 436-442. ArticlePubMedPMC
- 5. Yoo WS, Moon JS, Lee KO, Hwang SS, Koh JS, Lee HK, et al. 2009 National school health examination survey and analysis. Korean Educational Development Institute; 2010. Report No. CR 2010-38-1.
- 6. Yoo WS, Park SW, Kim JY, Park JH, Lee HS, Lee DH. 2011 National school health examination survey and analysis. Korean Educational Development Institute; 2011. Report No. CR2011-81.
- 7. Park SW, Hwang JH. Analysis of results and sampling study for the 2014 national school health examination of elementary, middle, and high school students. Korean Educational Development Institute; 2014. Report No. CR 2014-68.
- 8. Park SW, Moon JS, Hwang JH, Ryu DH. Analysis of results for the 2019 national school health examination of elementary, middle, and high school students. Ministry of Education, Korean Educational Environments Protection Agency; 2020. Report No. 2020 TR-11.
- 9. Kim DS, Shin HR, Chung DY, Moon JS, Lee KJ, Park SH, et al. Analysis of results for the 2024 national school health examination of elementary, middle, and high school students. Ministry of Education, Korean Educational Environments Protection Agency; 2025. Report No. 2025 TR-21.
- 10. Kim JH, Yun S, Hwang SS, Shim JO, Chae HW, Lee YJ, et al. The 2017 Korean National Growth Charts for children and adolescents: development, improvement, and prospects. Korean J Pediatr 2018; 61(5): 135-149. ArticlePubMedPMCLink
- 11. Bae JH, Lee SM, Kang HR. A study on the effectiveness evaluation of national health examinations for infants and children. National Health Insurance Service Health Insurance Policy Research Institute; 2018. Report No. 2018-1-0005.
- 12. Gwon D, Hwang JY, Oh J. Nutrition quotient for preschoolers and key impacting factors in Korea: a cross-sectional study on food literacy, social support, and the food environment of primary caregivers. Korean J Community Nutr 2025; 30(1): 16-26. ArticlePubMedPMCPDF
- 13. Han YH, Hyun T. Nutrient intake and food consumption of Korean preschool children: a comparison between a daycare meal group and non-daycare meal group using the data from the 2016-2019 Korea National Health and Nutrition Examination Survey. Nutr Res Pract 2025; 19(2): 225-240. ArticlePubMedPMCLink
- 14. Park E, Lee HY. Environment factors affecting childhood obesity: voices from students, parents, and teachers with photograph. J Korean Acad Nurs 2019; 49(3): 254-262. ArticlePubMedLink
- 15. Korea Disease Control and Prevention Agency (KDCA). Korea Health Statistics 2023: Korea National Health and Nutrition Examination Survey (KNHANES IX-2). KDCA; 2024 Dec. Report No. 11-1790387-000796-10.
- 16. Shingu College Industry-Academic Cooperation Foundation, National Institute of Food and Nutrition Service (NIFNS). Research on the dietary behavior survey of children and development of a dietary survey system by age group. National Institute of Food and Nutrition Service; 2023. Report No. 2024-01-030. 2023.
- 17. Yoon JH, Cho HY. A study on the historical development of school foodservice systems. Korean Educational Development Institute; 2016. Report No. CRM 2017-14.
- 18. Ministry of Education (MOE), Korean Educational Environments Protection Agency (KEEPA). A journey through time: school meals in photos and news. KEEPA; 2020.
- 19. Oh YM, Kim MH, Sung CJ. Effects of school lunch program on nutritional knowledge and attitude, and dietary behavior of Korean middle school students. Korean J Community Nutr 2005; 10(2): 163-173.
- 20. Kim Y, Son K, Kim J, Lee M, Park KH, Lim H. Associations between school lunch and obesity in Korean children and adolescents based on the Korea National Health and Nutrition Examination Survey 2017-2019 data: a cross-sectional study. Nutrients 2023; 15(3): 698.ArticlePubMedPMC
- 21. Kim S, Kim J, Chang H. Do types of snacks, sleep hours, and eating places affect nutritional intakes and its adequacy in adolescents? Nutr Res Pract 2021; 15(3): 396-410. ArticlePubMedPMCLink
- 22. Shim JS, Lee JM, Kim Y, Choi S, Oh K. Trends in dietary behavior of Korean adolescents: Korea youth risk behavior survey 2013-2022. Public Health Wkly Rep 2024; 17(37): 1563-1590. Article
- 23. Nam Y, Yoon J, Kim M. Application of draft nutritional standards for school lunches in the Republic of Korea: a feasibility study from the supplier perspective. Nutr Res Pract 2023; 17(1): 149-163. ArticlePubMedPMCLink
- 24. Park S, Um M, Kye S. Evaluation of nutrient intake and leftover food during school meal service among middle school students. J Learner Centered Curric Instruct 2022; 22(4): 13-26. Article
- 25. Lee KE. Students’ dietary habits, food service satisfaction, and attitude toward school meals enhance meal consumption in school food service. Nutr Res Pract 2019; 13(6): 555-563. ArticlePubMedPMCLink
- 26. Kang M, Park J, Kim Y, Son K, Park KH, Lim H. The BUDS (Balanced nUtrition through Daily School meals) program improved school meal intake and promoted healthy growth and eating behaviors in elementary school children. Nutr Res 2026; 148: 15-25. ArticlePubMed
- 27. Kim M, Kwon S, Hong SK, Koo Y, Lee Y. Development and application of an evaluation tool for school food culture in elementary, middle, and high schools in Gyeonggi Province, South Korea. Nutr Res Pract 2024; 18(5): 746-759. ArticlePubMedPMCLink
- 28. United Nations Economy and Social Council. Final report of the first executive board of the United Nations International Children’s Emergency Fund 11 December 1946-31 December 1950. United Nations International Children's Fund; 1951.
- 29. Jeong D. A historical analysis of maternal and child health programs in 1980s South Korea: insights from maternal and child health centers. Korean J Med Hist 2025; 34(1): 171-208. ArticlePubMedPMCPDF
- 30. Ministry of Health and Welfare (MOHW), Korea Health Promotion Institute (KHEPi). 20th Anniversary white paper of the NutriPlus program: with heart for twenty years, for the health of all. KHEPi; 2026.
- 31. Park OJ, Lee MJ, Kim JY, Min SH, Lee HS. The effect of nutrition plus program among 0~5 year children in the Yeojoo area: the improvement in nutritional status of children after nutrition supplement of children and nutrition education in parents/guardians. Korean J Community Nutr 2009; 14(6): 767-776.
- 32. Kang JH, Ryu HK. A study of the sustainability of NutriPlus program effect - in Pohang area -. Korean J Community Nutr 2011; 16(2): 206-214. Article
- 33. Park SA, Yoon EY. The effect of NutriPlus program among 1-5 year children in Daejeon area - the improvement in nutritional status of children and nutrition knowledge and attitude of parents -. Korean J Community Nutr 2013; 18(1): 1-10. Article
- 34. Kim YS, Kim SR, Jang YH, Kim DS, Kwon KH. A case study on effects of Nutrition-Plus program - based on infants and children under age 6 and their mothers in Naju region-. J Reg Stud 2011; 19(3): 143-163.
- 35. Kim HJ, Kim SH. The cost-benefit analysis of the NutriPlus program in Daejeon Dong-gu health center. Korean J Food Nutr 2015; 28(4): 717-727. Article
- 36. Ministry of Food and Drug Safety (MFDS). The 6th master plan for children’s dietary safety management (2025-2027) [Internet]. MFDS; 2024 [cited 2025 Nov 7]. Available from: https://www.mfds.go.kr/brd/m_218/view.do?seq=33617
- 37. Woo EY. Achievements and challenges of the center for children's foodservice management. Proceedings of 2020 Annual Conference of the Korean Society of Community Nutrition; 2020 Oct 16; Seoul: p. 307-330.
- 38. Kim HY, Yang IS, Chae IS, Yi BS, Park MK, Kim HY, et al. Effectiveness of center for child-care foodservice management for menu management and dietary variety. Korean J Community Nutr 2013; 18(3): 243-256. Article
- 39. Kim J, Han D, Oh J, Ryou HJ, Hwang JY, Kim K, et al. A study on the improvement of evaluation scheme for the installation and operation of center for children’s and social welfare foodservice management: utilizing interviews with center stakeholders and external experts. J Nutr Health 2024; 57(6): 685-698. ArticleLink
- 40. Ministry of Health and Welfare (MOHW), Ministry of Science and ICT, Ministry of Trade, Industry and Energy, Korea Disease Control and Prevention Agency. Operational management regulation for the national integrated bio big data project [Internet]. MOHW; 2024 [cited 2026 Mar 10]. Available from: https://www.mohw.go.kr/board.es?act=view&bid=0026&list_no=1480891&mid=a10409020000&nPage=4&tag=
- 41. BioBigData.Korea (BIKO). Project overview [Internet]. BIKO; n.d [cited 2026 Mar 10], Available from: https://www.biobigdata.kr/board?menuId=MENU002010100000000&siteId=SITE00002
- 42. Korean Law Information Center. Personal information protection act. Article 28-3 (restriction on combination of pseudonymous data) [Internet]. Ministry of Government Legislation; 2025 [cited 2026 Mar 10]. Available from: https://www.law.go.kr/DRF/lawService.do?OC=dl_lawinfosearch&target=law&MST=270351&type=HTML&mobileYn=&efYd=20251002
- 43. Korean Law Information Center. Enforcement decree of the personal information protection act. Article 29-3 (combination and release of pseudonymized information processed by different personal information controllers) [Internet]. Ministry of Government Legislation; 2025 [cited 2026 Mar 11]. Available from: https://www.law.go.kr/LSW/lsLinkCommonInfo.do?lspttninfSeq=159007&chrClsCd=010202
- 44. Park J, Son K, Woo S, Park KH, Lim H. A study on the relationship between the eating habits of elementary school students and the school meal intake measured by an artificial intelligence food scanner. J Korean Diet Assoc 2022; 28(4): 281-292. Article
- 45. Kim KY. AI food scanners for young children’s eating habits show high performance [Internet]. Daehan Foodservice News; 2024 Dec 16 [cited 2026 Mar 10]. Available from: http://www.fsnews.co.kr/news/articleView.html?idxno=55063
- 46. Choi YJ, Park SH. Korean food industry embraces AI to meet post-pandemic challenges [Internet]. The Chosun Daily; 2024 Apr 5 [cited 2026 Mar 11]. Available from: https://www.chosun.com/english/industry-en/2024/04/05/VQG6IKWAQ5GYBDNWJV5JJRYX5A/
- 47. Korean Law Information Center. Personal information protection act. Article 22-2 (protection of children’s personal information) [Internet]. Ministry of Government Legislation; 2025 [cited 2026 Mar 11]. Available from: https://www.law.go.kr/DRF/lawService.do?OC=dl_lawinfosearch&target=law&MST=270351&type=HTML&mobileYn=&efYd=20251002
- 48. Ministry of Science and ICT, Korea Information Society Development Institute. Human-centered “artificial intelligence (AI) ethical standards” [Internet]. Ministry of Science and ICT; 2020 [cited 2026 Mar 11]. Available from: https://nsp.nanet.go.kr/plan/subject/detail.do?nationalPlanControlNo=PLAN0000037532
- 49. World Health Organization (WHO). Ethics and governance of artificial intelligence for health. WHO; 2021.
- 50. United Nations (UN). Convention on the rights of the child. UN; 1989.
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteThe transition of nutritional status in infants, young children, and school-aged children in Korea and future-oriented nutritional strategies: a narrative review
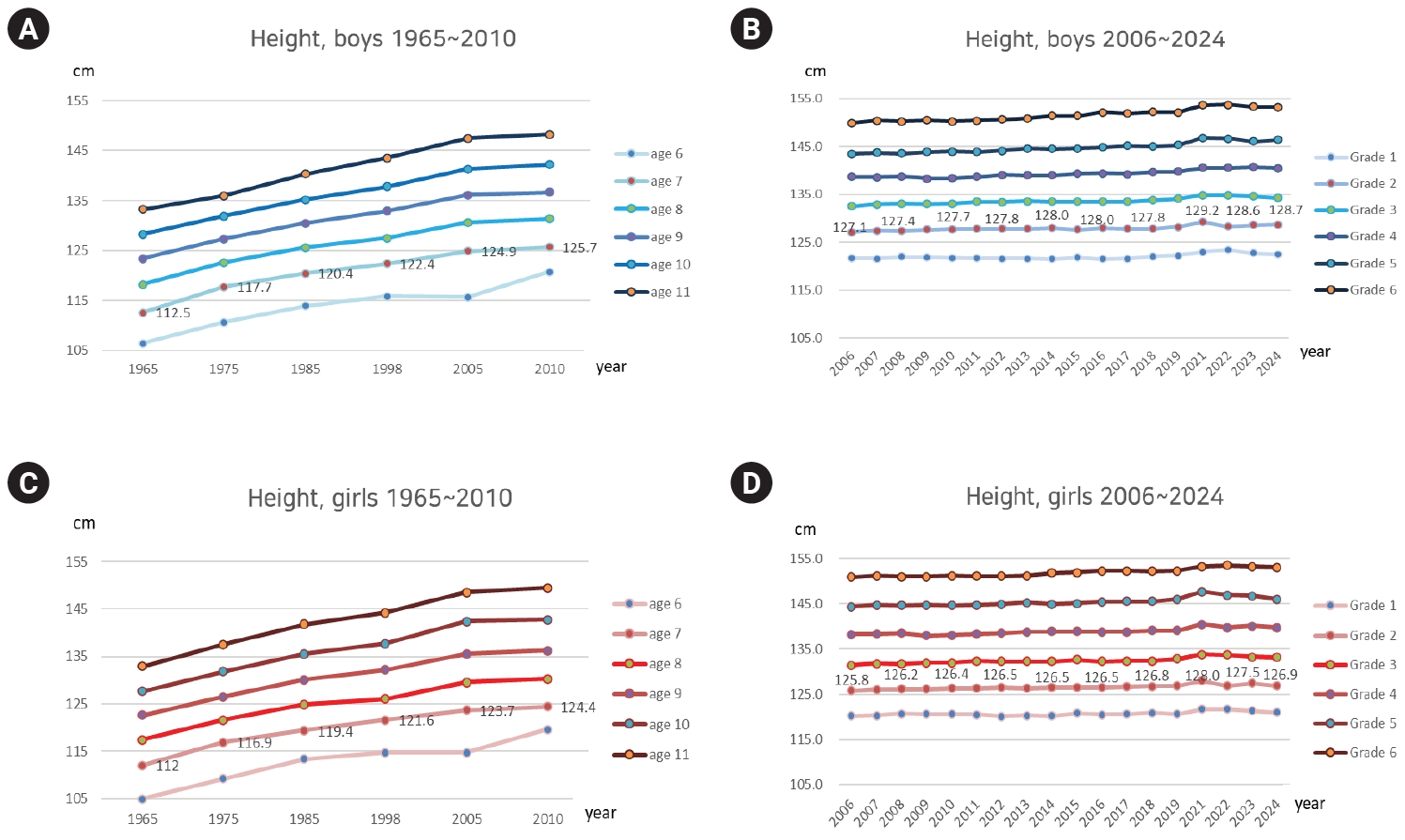
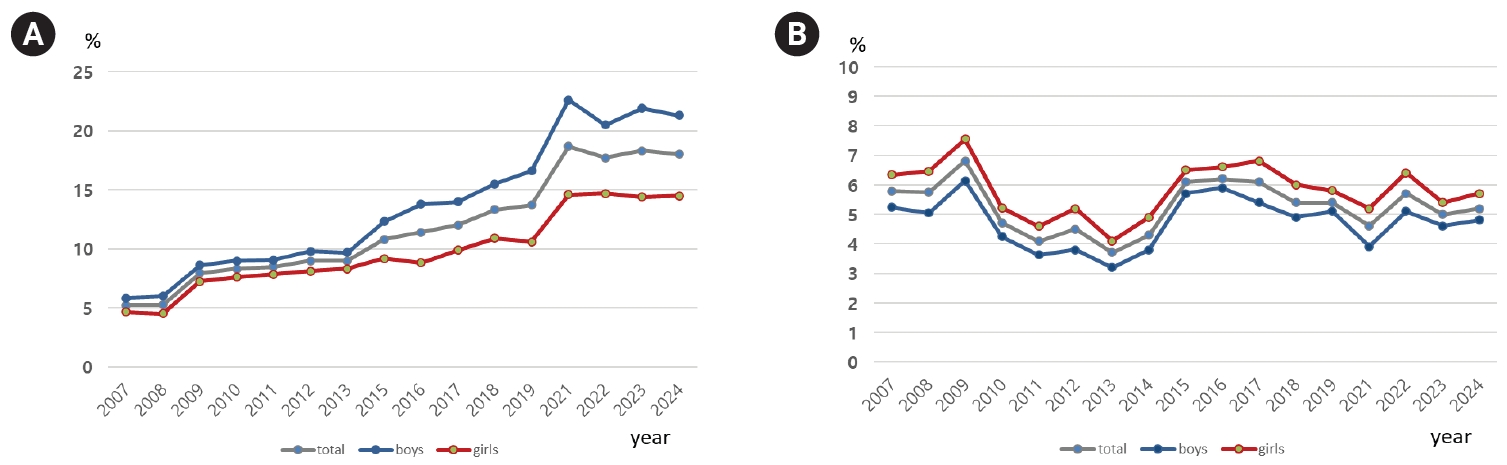
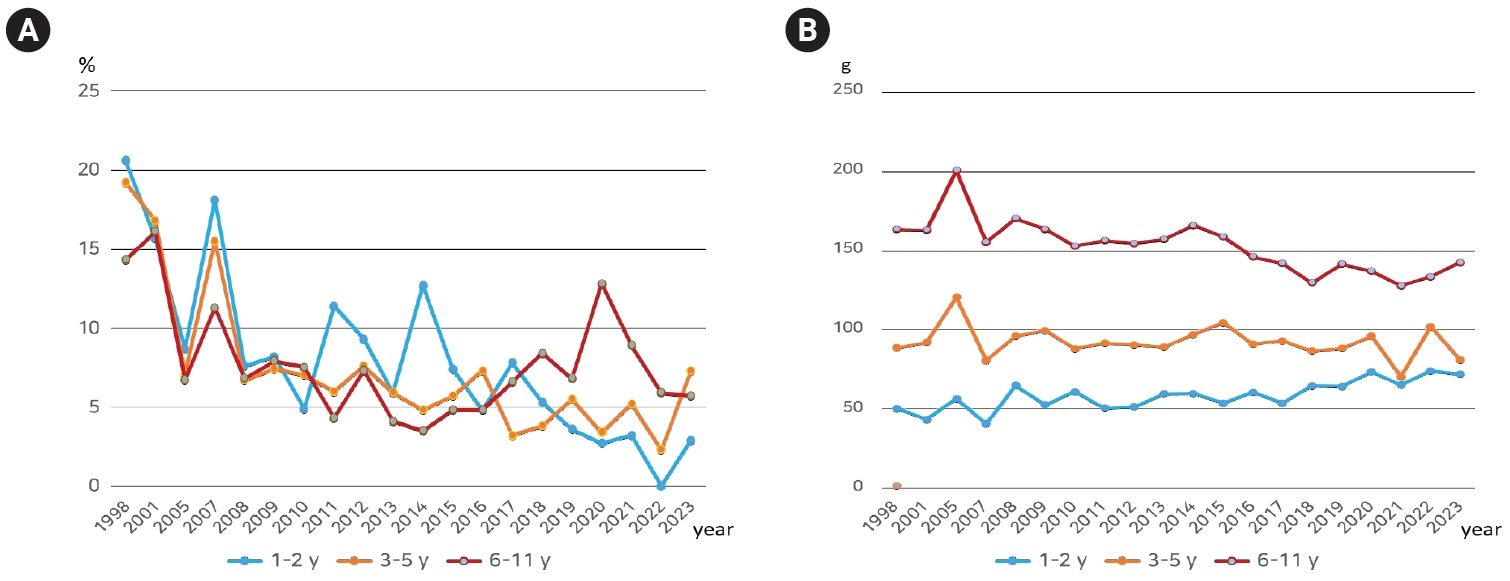
Fig. 1. Secular trends in the height of Korean children. (A, C) Anthropometric survey data by the Korean Pediatric Society and the Ministry of Health and Welfare [3,4]. (B, D) National school health examination data by the Ministry of Education [5-9].
Fig. 2. Long-term trends in the prevalence of obesity and underweight among Korean elementary school children. (A) Prevalence of obesity (BMI ≥ 95th percentile) (data by the Ministry of Education) [5-9]. (B) Prevalence of underweight (BMI < 5th percentile) (data by the Ministry of Education) [5-9]. BMI, body mass index.
Fig. 3. Long-term trends in the prevalence of inadequate nutrient and vegetable intake in Korean children. (A) Prevalence of inadequate nutrient intake: the proportion of the population whose energy intake is less than 75% of the estimated energy requirement and whose intake of calcium, iron, vitamin A, and riboflavin is less than the estimated average requirement, as reported in Korea Health Statistics 2023 [15]. (B) Vegetable intake as reported in Korea Health Statistics 2023 [15].
Fig. 1.
Fig. 2.
Fig. 3.
The transition of nutritional status in infants, young children, and school-aged children in Korea and future-oriented nutritional strategies: a narrative review
| Period | Nutrition policies for school-aged children | Nutrition policies for infants and young children |
|---|---|---|
| 1950–1970 | -Foreign aid-supported school feeding programs | -UNICEF milk powder and nutritional supplementation programs |
| -Maternal and child health services stipulated in the Public Health Center Act | ||
| 1970–1980 | -Transition to school-operated meal services and on-site meal preparation | |
| 1980–1990 | -Enactment of the School Meals Act | -Establishment of regional maternal and child health centers |
| 1990–2000 | -Nationwide expansion of school meal services | -Breastfeeding promotion programs, including the designation of baby-friendly hospitals |
| 2000–2010 | -Deployment of school nutrition teachers | -Introduction and nationwide expansion of the NutriPlus program |
| -Introduction of the school health promotion concept | -Enactment of the Special Act on Safety Management of Children’s Dietary Lifestyle | |
| -Enactment of the Special Act on Safety Management of Children’s Dietary Lifestyle | ||
| -Enactment of the Support for Diet Education Act | ||
| Since 2010 | -Expansion of free school meals | -Establishment and gradual expansion of the Center for Children’s Foodservice Management |
| -Comprehensive school meal safety measures | ||
| -Sodium reduction initiative | ||
| -Sugar reduction initiative |
Table 1. Historical overview of nutrition policies for school-aged children and infants/young children in Korea
UNICEF, United Nations Children’s Fund.


