
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 31(3); 2026 > Article
-
Review
- Life-course nutrition strategies for Korean middle-aged adults across biological transitions, nutritional burdens, and a community-linked precision nutrition model: a narrative review
-
Yoo Kyoung Park†

-
Korean Journal of Community Nutrition 2026;31(3):215-228.
DOI: https://doi.org/10.5720/kjcn.2026.00206
Published online: June 30, 2026
Professor, Department of Medical Nutrition, AgeTech-Service Convergence Major, Kyung Hee University, Yongin, Korea
- †Corresponding author: Yoo Kyoung Park Department of Medical Nutrition, AgeTech-Service Convergence Major, Kyung Hee University, 1732 Deokyeong-daero, Giheung-gu, Yongin 17104, Korea Tel: +82-31-201-3816 Fax: +82-31-203-3816 Email: ypark@khu.ac.kr
• Received: June 15, 2026 • Revised: June 25, 2026 • Accepted: June 26, 2026
© 2026 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 63 Views
- 3 Download
- Abstract
- INTRODUCTION
- METHODS
- DYNAMICS OF BIOLOGICAL AGING
- EPIDEMIOLOGY OF CHRONIC DISEASES IN KOREAN MIDDLE-AGED ADULTS
- IMBALANCE BETWEEN ENERGY INTAKE AND REQUIREMENTS AND DIET QUALITY DECLINE
- DIET QUALITY AND CHRONIC DISEASE RISK IN KOREAN MIDDLE-AGED ADULTS
- TAILORED NUTRITIONAL STRATEGIES FOR PHYSIOLOGICAL TRANSITIONS
- SYSTEMS-CENTERED, COMMUNITY-LINKED NUTRITION MODEL FOR MIDDLE-AGED ADULTS
- CONCLUSIONS
- NOTES
- REFERENCES
Abstract
-
Objectives
- To describe the nutritional challenges faced by Korean middle‑aged adults (40–64 years) from a life‑course and biological transition perspective and to propose systems‑based precision nutrition strategies for this critical stage of the lifespan.
-
Methods
- In this narrative review, PubMed, Medline, and Web of Science were searched for articles published between January 2010 and November 2025 using terms such as “middle aged nutrition,” “healthy aging,” “life course nutrition,” “sarcopenia,” “precision nutrition,” and “chronic diseases.” Policy documents and major national cohort and intervention studies were also reviewed.
-
Results
- Middle-aged adults in Korea have a high prevalence of chronic disease beginning in their 40s, showing “the triple burden of malnutrition:” obesity, insufficient micronutrients, and sarcopenia onset, along with excessive sodium and sugar consumption combined with socioeconomic factors like living alone. Nutrient and dietary approaches, such as high protein (1.2–1.5 g/kg/d), leucine, dairy products and fruits, anti-inflammatory foods intake, Dietary Approaches to Stop Hypertension (DASH) or Mediterranean diets plus lifestyle modification at public health centers (Korean Diabetes Prevention Study) for cardiometabolic risks, Mediterranean-DASH Intervention for Neurodegenerative Delay diet for cognition maintenance, could greatly impact health trajectories.
-
Conclusion
- Korean middle‑aged adults experience a triple burden of malnutrition on top of nonlinear biological aging shifts, which together accelerate cardiometabolic, musculoskeletal, and cognitive risks. Implementing targeted dietary strategies within a systems‑based, community‑linked precision nutrition model is essential to reshape health trajectories and promote healthy longevity in this population.
INTRODUCTION
METHODS
DYNAMICS OF BIOLOGICAL AGING
EPIDEMIOLOGY OF CHRONIC DISEASES IN KOREAN MIDDLE-AGED ADULTS
IMBALANCE BETWEEN ENERGY INTAKE AND REQUIREMENTS AND DIET QUALITY DECLINE
DIET QUALITY AND CHRONIC DISEASE RISK IN KOREAN MIDDLE-AGED ADULTS
TAILORED NUTRITIONAL STRATEGIES FOR PHYSIOLOGICAL TRANSITIONS
SYSTEMS-CENTERED, COMMUNITY-LINKED NUTRITION MODEL FOR MIDDLE-AGED ADULTS
Workplace and enterprise–centered environmental design
Expansion of preventive interventions in community health services
CONCLUSIONS
-
CONFLICT OF INTEREST
There are no financial or other issues that might lead to conflict of interest.
-
FUNDING
This research was supported by a grant from BK21 program “AgeTech- Service Convergence Major” through the National Research Foundation, funded by the Ministry of Education of Korea (Grant No. 5120200313836).
-
ACKNOWLEDGEMENTS
This study was based on a presentation delivered at the 2025 Fall Conference of the Korean Society of Community Nutrition.
-
DATA AVAILABILITY
This narrative review is based on previously published literature and does not contain original data.
NOTES
Fig. 1.Age-specific prevalence of chronic diseases. Adapted from Korea Health Statistics 2024: Korea National Health and Nutrition Examination Survey (KNHANES IX-3). Korea Disease Control and Prevention Agency, 2015 [8]. Hypertension: systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, or use of antihypertensive medication. Obesity: body mass index BMI ≥ 25 kg/m2 (Asia-Pacific criterion). Hypercholesterolemia: total cholesterol ≥ 240 mg/dL or use of cholesterol-lowering medication. Hypertriglyceridemia: fasting triglycerides ≥ 200 mg/dL. Diabetes mellitus (based on fasting glucose or HbA1c): fasting glucose ≥ 126 mg/dL, physician diagnosis, use of glucose-lowering medication or insulin, or HbA1c ≥ 6.5%.
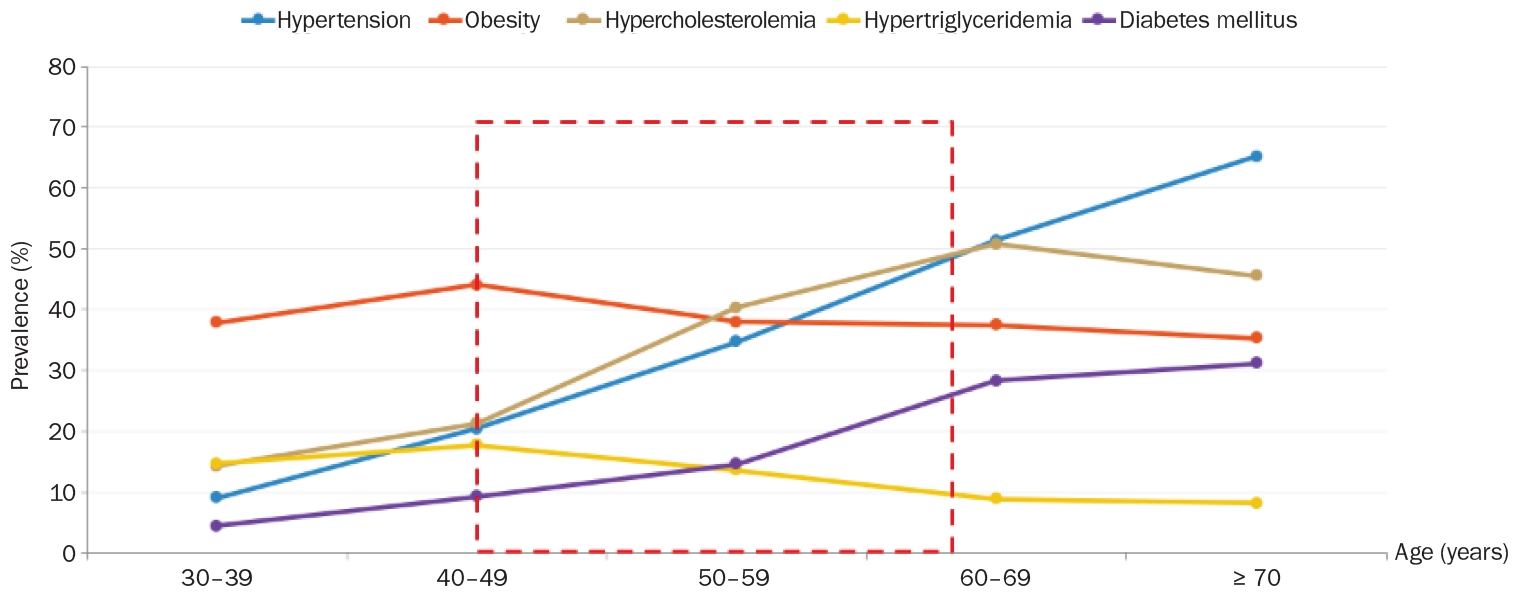
Table 1.Nonlinear dynamics of multi-omics profiles during human aging
Data from Shen et al. (Nat Aging 2024; 4(11): 1619-1634) [7].
Table 2.Nutrient intake status of Korean men aged 30–64 relative to 2025 KDRI
KNHANES, Korean national health and nutrition examination survey; KDRI, Korean Dietary Reference Intake; EER, estimated energy requirement; RNI, recommended nutrient intake; EAR, estimated average requirement; AMDR, acceptable macronutrient distribution range; CDRR, chronic disease risk reduction intake; AI, adequate intake.
Table 3.Nutrient intake status of Korean women aged 30–64 relative to 2025 KDRI
KNHANES, Korean national health and nutrition examination survey; KDRI, Korean Dietary Reference Intake; EER, estimated energy requirement; RNI, recommended nutrient intake; EAR, estimated average requirement; AMDR, acceptable macronutrient distribution range; CDRR, chronic disease risk reduction intake; AI, adequate intake.
Table 4.Key micronutrients and macronutrients for sarcopenia prevention
Table 5.Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet components for cognitive preservation
- 1. Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020; 139: 6-11. ArticlePubMedPMC
- 2. National Academy of Medicine, Commission for a Global Roadmap for Healthy Longevity. Global roadmap for healthy longevity. National Academies Press; 2022.
- 3. Lachman ME, Teshale S, Agrigoroaei S. Midlife as a pivotal period in the life course: balancing growth and decline at the crossroads of youth and old age. Int J Behav Dev 2015; 39(1): 20-31. ArticlePubMedPMC
- 4. Beckerman JP, Alike Q, Lovin E, Tamez M, Mattei J. The development and public health implications of food preferences in children. Front Nutr 2017; 4: 66.ArticlePubMedPMC
- 5. Infurna FJ, Gerstorf D, Lachman ME. Midlife in the 2020s: opportunities and challenges. Am Psychol 2020; 75(4): 470-485. ArticlePubMedPMC
- 6. Wagner C, Carmeli C, Jackisch J, Kivimäki M, van der Linden BWA, Cullati S, et al. Life course epidemiology and public health. Lancet Public Health 2024; 9(4): e261-e269. ArticlePubMed
- 7. Shen X, Wang C, Zhou X, Zhou W, Hornburg D, Wu S, et al. Nonlinear dynamics of multi-omics profiles during human aging. Nat Aging 2024; 4(11): 1619-1634. ArticlePubMedPMCPDF
- 8. Korea Disease Control and Prevention Agency (KDCA). Korea Health Statistics 2024: Korea National Health and Nutrition Examination Survey (KNHANES Ⅸ-3). KDCA; 2025 Dec. Report No. 11-1790387-000796-10.
- 9. Ministry of Health and Welfare, The Korean Nutrition Society. Dietary reference intakes for Koreans 2025. Ministry of Health and Welfare; 2025.
- 10. Yun S, Park S, Yook SM, Kim K, Shim JE, Hwang JY, et al. Development of the Korean Healthy Eating Index for adults, based on the Korea National Health and Nutrition Examination Survey. Nutr Res Pract 2022; 16(2): 233-247. ArticlePubMedPMCLink
- 11. Lee E, Kim JM. The association of the Korean Healthy Eating Index with chronic conditions in middle-aged single-person households. Nutr Res Pract 2023; 17(2): 316-329. ArticlePubMedPMCLink
- 12. An HJ, Chung SJ. Association between the Korean Healthy Eating Index sub-domains and the risk of metabolic syndrome in Korean adults: data from the 2022-2023 Korea National Health and Nutrition Examination Survey. Nutr Res Pract 2026; 20(1): 114-131. ArticlePubMedPMCLink
- 13. On S, Na W, Sohn C. Relationship between fermented food consumption patterns, hs-CRP, and chronic diseases among middle-aged Koreans: data from the 2015-2018 Korea National Health and Nutrition Examination. Nutrients 2025; 17(8): 1343.ArticlePubMedPMC
- 14. Tieland M, Trouwborst I, Clark BC. Skeletal muscle performance and ageing. J Cachexia Sarcopenia Muscle 2018; 9(1): 3-19. ArticlePubMedPMCLink
- 15. Ho-Pham LT, Nguyen HG, Nguyen-Pham SQ, Hoang DK, Tran TS, Nguyen TV. Longitudinal changes in bone mineral density during perimenopausal transition: the Vietnam Osteoporosis Study. Osteoporos Int 2023; 34(8): 1381-1387. ArticlePubMedPDF
- 16. El Khoudary SR, Nasr A. Cardiovascular disease in women: does menopause matter? Curr Opin Endocr Metab Res 2022; 27: 100419.ArticlePubMedPMC
- 17. Singh-Manoux A, Kivimaki M, Glymour MM, Elbaz A, Berr C, Ebmeier KP, et al. Timing of onset of cognitive decline: results from Whitehall II prospective cohort study. BMJ 2012; 344: d7622.ArticlePubMedPMC
- 18. Roberts SB, Silver RE, Das SK, Fielding RA, Gilhooly CH, Jacques PF, et al. Healthy aging-nutrition matters: start early and screen often. Adv Nutr 2021; 12(4): 1438-1448. ArticlePubMedPMCPDF
- 19. Jung S, Kang HJ, Choi M, Park YK. Toward a longevity diet framework: integrating global evidence for healthy aging in the South Korean population. Clin Nutr Res 2026; 15(2): 91-100. ArticlePubMedPMCPDF
- 20. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019; 48(1): 16-31. ArticlePubMedPMCPDF
- 21. Hong SH, Choi KM. Sarcopenic obesity, insulin resistance, and their implications in cardiovascular and metabolic consequences. Int J Mol Sci 2020; 21(2): 494.ArticlePubMedPMC
- 22. Roh E, Hwang SY, Kim JA, Lee YB, Hong SH, Kim NH, et al. Age- and sex-related differential associations between body composition and diabetes mellitus. Diabetes Metab J 2021; 45(2): 183-194. ArticlePubMedPMCPDF
- 23. Kim E, Chung S, Hwang J, Park YJ. 2020 Korean dietary reference intakes for protein: estimation of protein requirements and the status of dietary protein intake in the Korean population. J Nutr Health 2022; 55(1): 10-20. ArticleLink
- 24. Jung HW, Kim SW, Kim IY, Lim JY, Park HS, Song W, et al. Protein intake recommendation for Korean older adults to prevent sarcopenia: expert consensus by the Korean Geriatric Society and the Korean Nutrition Society. Ann Geriatr Med Res 2018; 22(4): 167-175. ArticlePubMedPMC
- 25. Han M, Woo K, Kim K. Association of protein intake with sarcopenia and related indicators among Korean older adults: a systematic review and meta-analysis. Nutrients 2024; 16(24): 4350.ArticlePubMedPMC
- 26. Kamei Y, Hatazawa Y, Uchitomi R, Yoshimura R, Miura S. Regulation of skeletal muscle function by amino acids. Nutrients 2020; 12(1): 261.ArticlePubMedPMC
- 27. Guasch-Ferré M, Satija A, Blondin SA, Janiszewski M, Emlen E, O’Connor LE, et al. Meta-analysis of randomized controlled trials of red meat consumption in comparison with various comparison diets on cardiovascular risk factors. Circulation 2019; 139(15): 1828-1845. ArticlePubMed
- 28. Nasimi N, Sohrabi Z, Nunes EA, Sadeghi E, Jamshidi S, Gholami Z, et al. Whey protein supplementation with or without vitamin D on sarcopenia-related measures: a systematic review and meta-analysis. Adv Nutr 2023; 14(4): 762-773. ArticlePubMedPMC
- 29. Weitzmann MN, Pacifici R. Estrogen deficiency and bone loss: an inflammatory tale. J Clin Invest 2006; 116(5): 1186-1194. ArticlePubMedPMC
- 30. Ahn SH, Park SM, Park SY, Yoo JI, Jung HS, Nho JH, et al. Osteoporosis and osteoporotic fracture fact sheet in Korea. J Bone Metab 2020; 27(4): 281-290. ArticlePubMedPMCPDF
- 31. Shin S, Joung H. A dairy and fruit dietary pattern is associated with a reduced likelihood of osteoporosis in Korean postmenopausal women. Br J Nutr 2013; 110(10): 1926-1933. ArticlePubMed
- 32. Na W, Park S, Shivappa N, Hébert JR, Kim MK, Sohn C. Association between inflammatory potential of diet and bone-mineral density in Korean postmenopausal women: data from fourth and fifth Korea National Health and Nutrition Examination Surveys. Nutrients 2019; 11(4): 885.ArticlePubMedPMC
- 33. Kim DE, Cho SH, Park HM, Chang YK. Relationship between bone mineral density and dietary intake of β-carotene, vitamin C, zinc and vegetables in postmenopausal Korean women: a cross-sectional study. J Int Med Res 2016; 44(5): 1103-1114. ArticlePubMedPMCLink
- 34. Yin F, Sancheti H, Patil I, Cadenas E. Energy metabolism and inflammation in brain aging and Alzheimer's disease. Free Radic Biol Med 2016; 100: 108-122. ArticlePubMedPMC
- 35. Morris MC, Tangney CC, Wang Y, Sacks FM, Barnes LL, Bennett DA, et al. MIND diet slows cognitive decline with aging. Alzheimers Dement 2015; 11(9): 1015-1022. ArticlePubMedPMCLink
- 36. Morris MC, Tangney CC, Wang Y, Sacks FM, Bennett DA, Aggarwal NT. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement 2015; 11(9): 1007-1014. ArticlePubMedPMCLink
- 37. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, et al.; DASH Collaborative Research Group. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med 1997; 336(16): 1117-1124. ArticlePubMed
- 38. Estruch R, Ros E, Salas-Salvadó J, Covas MI, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med 2018; 378(25): e34.ArticlePubMed
- 39. Zhang J, Lu X, Wu R, Ni H, Xu L, Wu W, et al. Associations between composite dietary antioxidant index and estimated 10-year atherosclerotic cardiovascular disease risk among U.S. adults. Front Nutr 2023; 10: 1214875.ArticlePubMedPMC
- 40. Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet 2012; 379(9833): 2279-2290. ArticlePubMedPMC
- 41. Abate N, Chandalia M. Risk of obesity-related cardiometabolic complications in special populations: a crisis in Asians. Gastroenterology 2017; 152(7): 1647-1655. ArticlePubMed
- 42. Rhee SY, Chon S, Ahn KJ, Woo JT; Korean Diabetes Prevention Study Investigators. Hospital-Based Korean Diabetes Prevention Study: a prospective, multi-center, randomized, open-label controlled study. Diabetes Metab J 2019; 43(1): 49-58. ArticlePubMedPMCLink
- 43. Park JH, Park JH. Digital health literacy, health empowerment, and health promotion behaviors among middle-aged women. J Muscle Jt Health 2024; 31(3): 137-145. Article
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteLife-course nutrition strategies for Korean middle-aged adults across biological transitions, nutritional burdens, and a community-linked precision nutrition model: a narrative review
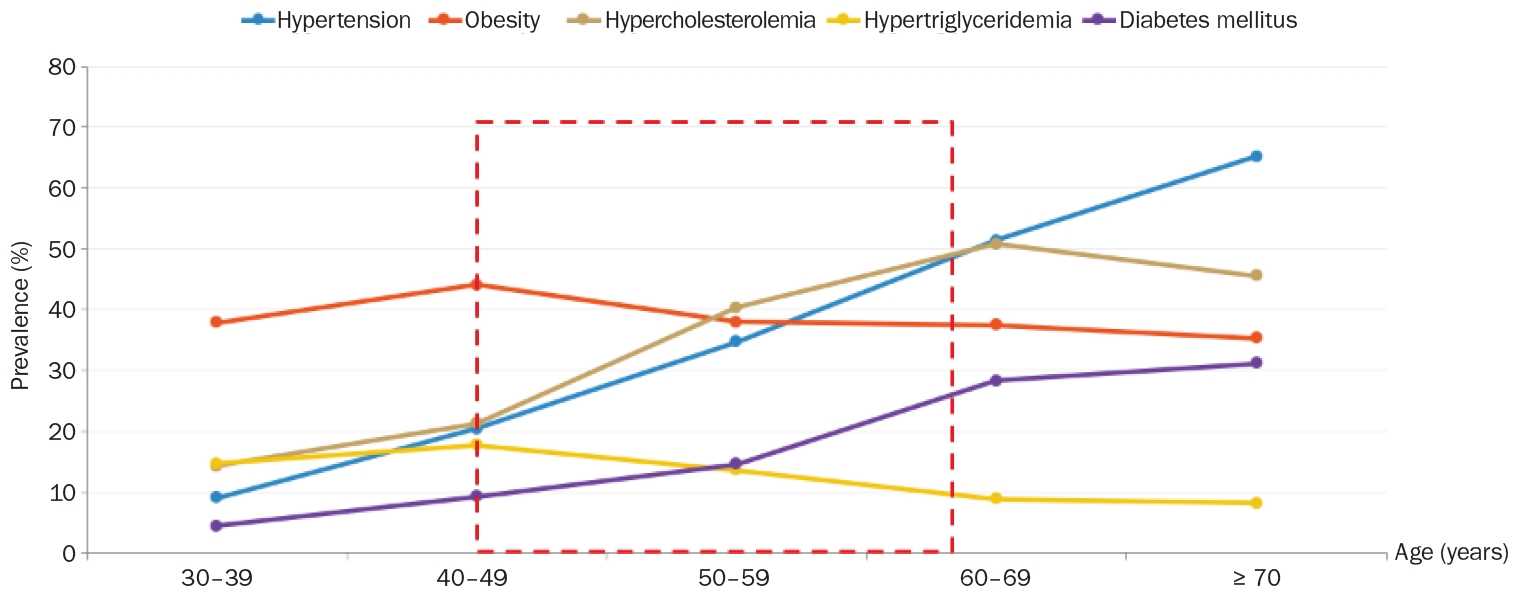
Fig. 1. Age-specific prevalence of chronic diseases. Adapted from Korea Health Statistics 2024: Korea National Health and Nutrition Examination Survey (KNHANES IX-3). Korea Disease Control and Prevention Agency, 2015 [8]. Hypertension: systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, or use of antihypertensive medication. Obesity: body mass index BMI ≥ 25 kg/m2 (Asia-Pacific criterion). Hypercholesterolemia: total cholesterol ≥ 240 mg/dL or use of cholesterol-lowering medication. Hypertriglyceridemia: fasting triglycerides ≥ 200 mg/dL. Diabetes mellitus (based on fasting glucose or HbA1c): fasting glucose ≥ 126 mg/dL, physician diagnosis, use of glucose-lowering medication or insulin, or HbA1c ≥ 6.5%.
Fig. 1.
Life-course nutrition strategies for Korean middle-aged adults across biological transitions, nutritional burdens, and a community-linked precision nutrition model: a narrative review
| Biological aging crest | Approximate chronological age | Primary molecular & metabolic dysregulation | Clinical implications & associated risks |
|---|---|---|---|
| Crest 1 (early midlife transition) | 44 years | Lipid metabolism | Hyperlipidemia |
| Alcohol metabolism | Early atherosclerosis | ||
| Structural proteins in the skin and muscle | Metabolic syndrome | ||
| Cardiovascular disease pathways | Decline in muscle elasticity | ||
| Skin aging | |||
| Crest 2 (late midlife transition) | 60 years | Immune regulation | Immunosenescence |
| Carbohydrate metabolism | Type 2 diabetes onset | ||
| Oxidative phosphorylation | Profound loss of bone mineral density (osteoporosis) | ||
| Kidney function pathways | Accelerated sarcopenia |
| Nutrient | Age (year) | DRI | Mean intake (based on KNHANES 2013–2022) | Below the KDRI (%) |
|---|---|---|---|---|
| Energy (kcal/d) | 30–49 | EER: 2,500 | ~2,500 | - |
| 50–64 | EER: 2,200 | ~2,100–2,200 | - | |
| Protein (g/d) | 30–49 | RNI: 65 | 88.8 | 13.8 |
| EAR: 50 | ||||
| 50–64 | RNI: 60 | 80.6 | 21.1 | |
| EAR: 50 | ||||
| Fat (%/E) | 30–49 | AMDR: 15–30 | 20.7 | - |
| 50–64 | 16.7 | - | ||
| Saturated fatty acid (%/E) | 19–64 | CDRR: < 7% | Generally < 7% | - |
| Sugars (g/d) | 30–49 | Goal: < 20% of total energy | 63.3 | - |
| 50–64 | 60.8 | - | ||
| Calcium (mg/d) | 30–49 | RNI: 800 | 495.7 (median) | 71.4 |
| EAR: 650 | ||||
| 50–64 | RNI: 750 | 517.0 (median) | 64.6 | |
| EAR: 600 | ||||
| Vitamin D (μg/d) | 30–49 | AI: 10 | 3.5 | 92.6 |
| 50–64 | 4.0 | 92.1 | ||
| Vitamin A (μg RAE/d) | 30–49 | RNI: 800 | 410.6 | 78.8 |
| EAR: 560 | ||||
| 50–64 | RNI: 750 | 458.8 | 74.4 | |
| EAR: 530 | ||||
| Riboflavin (mg/d) | 30–49 | RNI: 1.5 | 1.91 | 29.0 |
| 50–64 | EAR: 1.3 | 1.75 | 34.1% | |
| Sodium (mg/d) | 30–49 | AI: 1,500 | 4,026.0 | Above CDRR: 83.4 |
| CDRR: 2,300 | Below AI: 5.0 | |||
| 50–64 | 3,942.2 | Above CDRR: 79.4 | ||
| Below AI: 5.3 |
| Nutrient | Age (year) | DRI | Mean intake (based on KNHANES 2013–2022) | Below the KDRI (%) |
|---|---|---|---|---|
| Energy (kcal/d) | 30–49 | EER: 1,900 | ~1,800–1,900 | - |
| 50–64 | EER: 1,700 | ~1,500–1,600 | - | |
| Protein (g/d) | 30–49 | RNI: 50 | 59.5 | 24.2 |
| EAR: 40 | ||||
| 50–64 | RNI: 60 | 59.3 | 22.6 | |
| EAR: 50 | ||||
| Fat (%/E) | 30–49 | AMDR: 15–30 | 21.1 | - |
| 50–64 | 17.5 | - | ||
| Saturated fatty acid (%/E) | 19–64 | CDRR: < 7% | Generally < 7% | - |
| Sugars (g/d) | 30–49 | Goal: < 20% of total energy | 50.8 | - |
| 50–64 | 61.5 | - | ||
| Calcium (mg/d) | 30–49 | RNI: 700 | 397.1 (median) | 74.0 |
| 50–64 | EAR: 580 | 437.1 (median) | 72.8 | |
| Vitamin D (μg/d) | 30–49 | AI: 10 | 2.6 | 95.6 |
| 50–64 | 3.1 | 95.5 | ||
| Vitamin A (μg RAE/d) | 30–49 | RNI: 650 | 350.2 | 76.2 |
| EAR: 450 | ||||
| 50–64 | RNI: 600 | 379.6 | 70.7 | |
| EAR: 430 | ||||
| Riboflavin (mg/d) | 30–49 | RNI: 1.2 | 1.41 | 31.0 |
| 50–64 | EAR: 1.0 | 1.40 | 29.1 | |
| Sodium (mg/d) | 30–49 | AI: 1,500 | 2722.6 | Above CDRR: 55.4 |
| CDRR: 2,300 | Below AI: 17.5 | |||
| 50–64 | 2769.2 | Above CDRR: 55.6 | ||
| Below AI: 17.5 |
| Target nutrient | Recommended intake dose for muscle preservation | Physiological role in middle-aged adults |
|---|---|---|
| Total dietary protein | 1.2–1.5 g/kg/day (or 25–30 g/meal) | Overcomes anabolic resistance and provides primary building blocks for muscle protein synthesis |
| Leucine (branched-chain amino acids) | 2.5–3.0 g/meal | Direct activator of the mTORC1 signaling pathway, initiating muscle anabolism |
| Vitamin D | 800–1,000 IU/day | Upregulates intramuscular vitamin D receptors and enhances fast-twitch muscle fiber function |
| Magnesium | 300 mg/day (men), 270 mg/day (women) | Co-factor in ATP synthesis and insulin signaling; mitigates age-related muscle mass loss |
| Vitamin C/E | 45–90 mg/day (vitamin C), 400 IU/day (vitamin E) | Decreases reactive oxygen species that exacerbate age-related muscle catabolism |
| Dietary component | MIND diet recommendation | Neuroprotective mechanism |
|---|---|---|
| Green leafy vegetables | ≥ 6 servings/week | Rich in folate, lutein, and vitamin K; suppresses neuroinflammation and maintains synaptic plasticity |
| Berries | ≥ 2 servings/week | Contains anthocyanins that promote neural signal transmission in the cerebral cortex and defend against oxidative stress |
| Extra virgin olive oil | Primary cooking fat | Oleocanthal activates the clearance of amyloid-beta (Aβ) plaques, which induce Alzheimer’s |
| Nuts & fish | Nuts ≥ 5 servings/week | Omega-3 (EPA, DHA) unsaturated fatty acids preserve brain cell membrane fluidity and protect microvessels |
| Fish ≥ 1 serving/week | ||
| Red meat & fast food | Red meat < 4 servings/week | Blocks generation of saturated fats and advanced glycation end-products, preventing damage to blood-brain barrier permeability |
| Fried food < 1 serving/week |
Table 1. Nonlinear dynamics of multi-omics profiles during human aging
Data from Shen
Table 2. Nutrient intake status of Korean men aged 30–64 relative to 2025 KDRI
KNHANES, Korean national health and nutrition examination survey; KDRI, Korean Dietary Reference Intake; EER, estimated energy requirement; RNI, recommended nutrient intake; EAR, estimated average requirement; AMDR, acceptable macronutrient distribution range; CDRR, chronic disease risk reduction intake; AI, adequate intake.
Table 3. Nutrient intake status of Korean women aged 30–64 relative to 2025 KDRI
KNHANES, Korean national health and nutrition examination survey; KDRI, Korean Dietary Reference Intake; EER, estimated energy requirement; RNI, recommended nutrient intake; EAR, estimated average requirement; AMDR, acceptable macronutrient distribution range; CDRR, chronic disease risk reduction intake; AI, adequate intake.
Table 4. Key micronutrients and macronutrients for sarcopenia prevention
Data from Kamei Data from Guasch-Ferré Data from Nasimi
Table 5. Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet components for cognitive preservation


