
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 29(6); 2024 > Article
-
Research Article
일차의료 연계 2형당뇨병 환자를 위한 영양교육 프로그램 적용 효과: pilot 중재연구 -
양혜림1),*
 , 박유경2),*, 이지현3), 임희숙4), 백희준5), 이혜진6), 박해란7), 이평화8), 정주연9), 김원경10),†
, 박유경2),*, 이지현3), 임희숙4), 백희준5), 이혜진6), 박해란7), 이평화8), 정주연9), 김원경10),† - Impact of a public health center nutrition education program on patients with type 2 diabetes in a primary care-based chronic disease management project: a pilot intervention study
-
Haerim Yang1),*, Yoo Kyoung Park2),*, Ji-hyun Lee3), Hee-Sook Lim4), Heejoon Baek5), Hyejin Lee6), Haeran Park7), Pyunghwa Lee8), Jooyoun Chung9), Won Gyoung Kim10),†
-
Korean Journal of Community Nutrition 2024;29(6):492-503.
DOI: https://doi.org/10.5720/kjcn.2024.00018
Published online: December 31, 2024
1)경희대학교 동서의학대학원 의학영양학과 학생
2)경희대학교 동서의학대학원 의학영양학과 교수
3)아주대학교병원 영양팀장
4)경희대학교 동서의학대학원 노인학과 고령서비스-테크 융합전공 부교수
5)한양여자대학교 식품영양과 조교수
6)대구시 공공보건의료지원단 부단장
7)양산시 보건소 영양사
8)한국건강증진개발원 주임전문원
9)한국건강증진개발원 팀장
10)신구대학교 식품영양학과 조교수
1)Graduate Student, Department of Medical Nutrition, Graduate School of East-West Medical Science, Kyung Hee University, Yongin, Korea
2)Professor, Department of Medical Nutrition, Graduate School of East-West Medical Science, Kyung Hee University, Yongin, Korea
3)Team Leader, Clinical Nutrition Team, Ajou University Hospital, Suwon, Korea
4)Associate Professor, AgeTech-Service Convergence Major, Department of Gerontology, Graduate School of East-West Medical Science, Kyung Hee University, Yongin, Korea
5)Assistant Professor, Department of Food and Nutrition, Hanyang Women’s University, Seoul, Korea
6)Vice-Director, Daegu Public Health Policy Institute, Daegu, Korea
7)Dietitian, Yangsan Public Health Center, Yangsan, Korea
8)Associate Officer, Health Promotion Institute, Seoul, Korea
9)Team Manager, Health Promotion Institute, Seoul, Korea
10)Assistant Professor, Department of Food and Nutrition, Shingu College, Seongnam, Korea
- †Corresponding author: Won Gyoung Kim Department of Food and Nutrition, Shingu College, 377 Gwangmyeong-ro, Jungwon-gu, Seongnam 13174, Korea Tel: +82-31-740-1678 Fax: +82-31-740-1590 Email: nury86@shingu.ac.kr
• Received: June 17, 2024 • Revised: September 30, 2024 • Accepted: October 21, 2024
© 2024 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,404 Views
- 111 Download
Abstract
-
Objectives
- We investigated the impact of an advanced “Nutrition Education Program” on patients with Diabetes mellitus, type 2 from public health centers enrolled in a primary health care-based chronic disease management project. This 12-week dietary management program was developed by the Korea Health Promotion and Development Institute. We assessed if this program improved glycemic control and other health indicators through dietary and nutritional improvements.
-
Methods
- Seventeen patients with Diabetes mellitus type 2 were enrolled in the “Nutrition Education Program.” These patients were referred to public health centers for lifestyle management based on physician assessments at local clinics that were participating in a pilot project on primary health care-based chronic disease management. The participants attended the program comprising face-to-face basic, in-depth, and practical training sessions at the health center during the third, fifth, and seventh weeks, respectively. Anthropometric measurements, body composition analysis, blood biochemical characteristics, nutritional knowledge, and self-efficacy evaluation were performed before and after the program. Data were analyzed using SPSS ver. 28.0.
-
Results
- The mean age of the participants was 62 years, and most participants were female (14, 82.4%). No significant changes in patients’ anthropometric measurements or body composition were observed after the training. However, significant reductions were observed in the blood biochemical characteristics, including glycated hemoglobin, total cholesterol, and low-density lipoprotein levels. Additionally, patients’ nutritional knowledge and self-efficacy scores increased significantly.
-
Conclusions
- The “Nutrition Education Program” helped in improving glycemic control and other health indicators in patients with Diabetes mellitus type 2. Further research is required to objectively confirm the long-term and sustained effects of the program in a controlled study.
-
Trial Registration
- Clinical Research Information Service Identifier: KCT0010010.
INTRODUCTION
METHODS
1) 환자 연계 및 12주 식생활 관리 프로그램
2) 일반적인 특성
3) 신체계측 및 체성분 특성
4) 혈액생화학적 특성
5) 영양지식 평가
6) 자기효능감 평가
RESULTS
DISCUSSION
-
CONFLICT OF INTEREST
There are no financial or other issues that might lead to conflict of interest.
-
FUNDING
This study was supported by a grant from the Korea Health Promotion and Development Institute.
-
DATA AVAILABILITY
Research data is available upon a reasonable request to the corresponding author.
NOTES
Fig. 1.Procedure for nutrition education program in collaboration between a clinic and public health center.
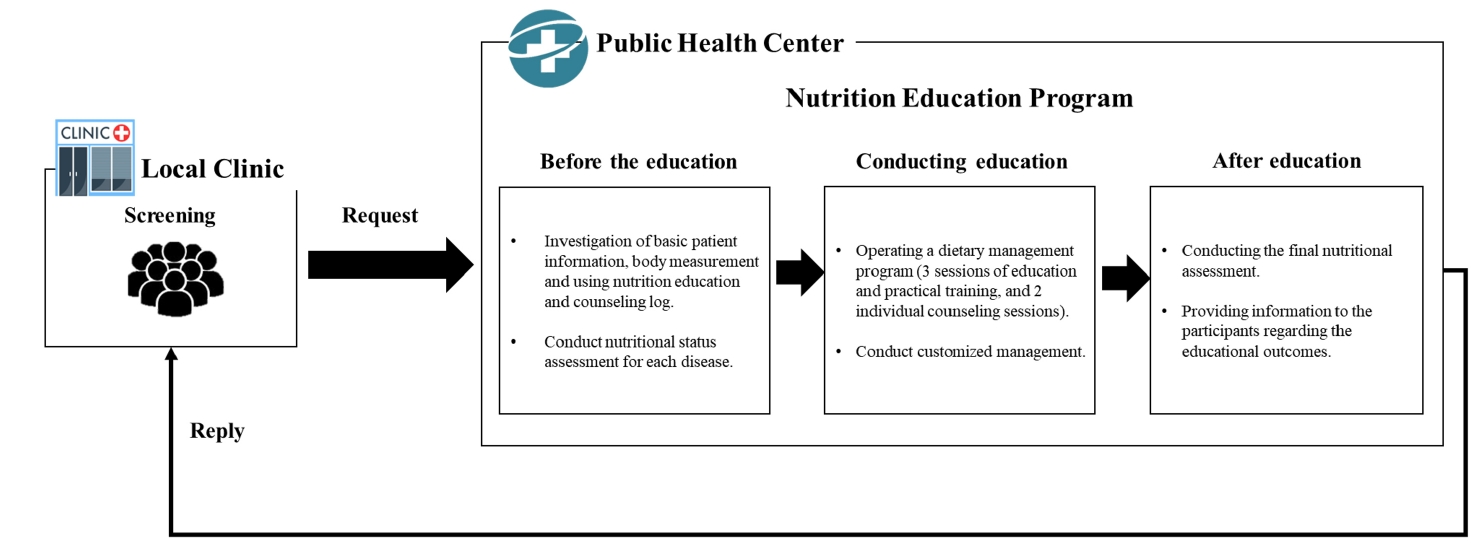
Table 1.12-Week dietary lifestyle management program for diabetes patients
| Week | Section | Content | Method |
|---|---|---|---|
| 1 | Pre-assessment and evaluation | • Conducting a nutritional status assessment | Online |
| • Subject basic information and dietary habits survey, etc. | |||
| 2 | ① Customized management | • Guidance for the first session of nutritional education | Online |
| • Encouragement for participation, and the like | |||
| 31) | 1st basic nutrition education | • Implementation of basic education | Face to face |
| [The Basic principles of dietary management for diabetic patients] | |||
| - Diabetes mellitus etiology | |||
| - The significance of dietary therapy | |||
| - Diabetes and its complications | |||
| - Eating a balanced diet regularly | |||
| • Results of the first education and personalized management feedback | |||
| 4 | ② Customized management | • Guidance on the second session of nutritional education | Online |
| • Blood sugar check | |||
| 51) | 2nd in-depth nutrition education | • Conduct in-depth training | Face to face |
| [Blood glucose management in special circumstances] | |||
| - When sick, when exercising, and blood sugar management | |||
| - Symptoms and management of hypoglycemia | |||
| - Considerations for popular folk remedies, etc. | |||
| • Results feedback from the second session of education and personalized management | |||
| 6 | ③ Customized management | • Guidance on the third session of nutritional practicum education | Online |
| • Education content reminding | |||
| 71) | 3rd practical training1) | • Guidance for the Third Session of nutritional practical training | Face to face |
| [Diabetes taste testing event] | |||
| - Portion control experiment with personal meal size | |||
| - Exploring adequate meal portions for myself | |||
| 8 | ④ Customized management | • Personal consultation guide | Online |
| • Blood sugar check | |||
| 9 | 4th individual consultation | • Conduct individual education and counseling | Online |
| • Results feedback from the fourth session of counseling and personalized management | |||
| 10 | ⑤ Customized management | • Counseling content reminding | Online |
| • Question and answer session | |||
| 11 | ⑥ Customized management | • Personal consultation guide | Online |
| • Blood sugar check | |||
| 12 | 5th individual consultation | • Conducting individual education and counseling | Online |
| • The end of the program | |||
| • Final management results feedback |
Table 2.Baseline characteristics of patients
| Variable | Participant (n = 17) |
|---|---|
| Sex | |
| Male | 3 (17.6) |
| Female | 14 (82.4) |
| Age (year) | 62.71 ± 6.56 |
| 19–64 | 10 (58.8) |
| ≥ 65 | 7 (41.2) |
| Classification of obesity1) | |
| Normal | 1 (5.9) |
| Overweight | 11 (64.7) |
| Obesity | 5 (29.4) |
Table 3.Changes in anthropometric and body composition characteristics after diabetes education
| Variable |
Participant (n = 17) |
P-value1) | |
|---|---|---|---|
| Before | After | ||
| Weight (kg) | 63.5 ± 10.3 | 63.7 ± 10.8 | 0.918 |
| BMI (kg/m2) | 25.1 ± 2.3 | 25.1 ± 2.5 | 0.850 |
| Waist circumference (cm) | 88.3 ± 7.3 | 89.1 ± 8.1 | 0.582 |
| Body fat mass (kg) | 21.8 ± 5.8 | 21.0 ± 5.6 | 0.231 |
| Percent body fat (%) | 33.4 ± 3.9 | 33.1 ± 4.0 | 0.209 |
| Muscle mass (kg) | 38.4 ± 6.2 | 38.7 ± 6.4 | 0.378 |
| SBP (mm/Hg) | 117.7 ± 11.0 | 116.9 ± 13.5 | 0.850 |
| DBP (mm/Hg) | 71.2 ± 7.8 | 71.2 ± 19.0 | 0.314 |
Table 4.Changes in blood biochemistry after diabetes education
| Variable |
Participant (n = 17) |
P-value1) | |
|---|---|---|---|
| Before | After | ||
| Fasting plasma glucose (mg/dL) | 123.1 ± 21.0 | 119.8 ± 23.3 | 0.981 |
| HbA1c (%) | 6.5 ± 0.5 | 6.4 ± 0.5 | 0.029 |
| Cholesterol | |||
| Total cholesterol (mg/dL) | 166.4 ± 49.7 | 151.9 ± 37.7 | 0.047 |
| LDL-cholesterol (mg/dL) | 82.6 ± 38.8 | 56.9 ± 22.4 | 0.014 |
| HDL-cholesterol (mg/dL) | 58.7 ± 16.3 | 61.1 ± 15.7 | 0.066 |
| Triglyceride (mg/dL) | 132.6 ± 64.4 | 175.6 ± 73.4 | 0.074 |
Table 5.Changes in nutrition knowledge questionnaire after diabetes education
| Nutrition knowledge |
Participant (n = 17) |
P-value1) | |
|---|---|---|---|
| Before | After | ||
| Diabetes is caused by a deficiency or lack of insulin. | 7.7 ± 4.4 | 10.0 ± 0.0 | 0.046 |
| The medication is more crucial than diet or exercise in the treatment of diabetes. | 5.3 ± 5.1 | 9.4 ± 2.4 | 0.008 |
| If there are no specific symptoms, treatment may not be necessary for diabetes. | 8.2 ± 3.9 | 10.0 ± 0.0 | 0.083 |
| If blood sugar levels continue to rise, it can lead to visual impairment or impaired kidney function. | 10.0 ± 0.0 | 10.0 ± 0.0 | > 0.999 |
| If there is a high risk of low blood sugar, it is possible to consume a pre-exercise snack. | 10.0 ± 0.0 | 10.0 ± 0.0 | > 0.999 |
| After taking diabetes medication or receiving an insulin injection, if symptoms such as cold sweats, palpitations, hunger, fatigue, trembling hands, and headache occur, patients with diabetes should consume one tablespoon of sugar (15 g). | 9.4 ± 2.4 | 10.0 ± 0.0 | 0.317 |
| Maintaining a normal body weight is important for blood sugar control. | 10.0 ± 0.0 | 10.0 ± 0.0 | > 0.999 |
| Diabetic patients should not forego blood sugar monitoring and meals, as hypoglycemia may occur after alcohol consumption. | 7.7 ± 4.3 | 10.0 ± 0.0 | 0.046 |
| Fruits and vegetables contribute to lowering blood sugar levels. | 5.3 ± 5.1 | 7.1 ± 4.7 | 0.083 |
| Mixed grain rice can be consumed in larger quantities compared to white rice. | 7.1 ± 4.7 | 9.4 ± 2.4 | 0.046 |
| Nutritional knowledge total score | 80.6 ± 15.2 | 95.9 ± 6.2 | < 0.001 |
Table 6.Changes in self-efficacy after diabetes education
| Component |
Participant (n = 17) |
P-value1) | |
|---|---|---|---|
| Before | After | ||
| I can adhere to dietary practices for blood pressure and blood sugar control. | 3.9 ± 1.0 | 4.1 ± 0.8 | 0.157 |
| I can control the amount of meals and keep it constant. | 3.5 ± 0.8 | 4.2 ± 0.8 | 0.002 |
| I can visit the clinic regularly to check the condition of the disease and get a complication check. | 4.2 ± 0.7 | 4.4 ± 0.6 | 0.046 |
| I can maintain normal blood pressure and blood sugar levels. | 3.7 ± 0.9 | 4.1 ± 0.8 | 0.035 |
| I can keep my body weight constant. | 3.9 ± 0.7 | 3.9 ± 0.7 | > 0.999 |
| I can manage stress or anxiety just as effectively as during normal times. | 3.4 ± 0.8 | 3.8 ± 0.9 | 0.070 |
| I can ask my family for help when I have poor blood pressure/blood sugar control. | 3.5 ± 0.9 | 4.1 ± 0.7 | 0.015 |
| I can always practice eating blandly. | 3.8 ± 1.2 | 4.2 ± 0.9 | 0.023 |
| Self-efficacy total score | 29.7 ± 5.0 | 32.8 ± 5.2 | 0.002 |
- 1. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract 2022; 183: 109119.ArticlePubMedPMC
- 2. Moon JS. Revisiting the diabetes crisis in Korea: call for urgent action. J Korean Diabetes 2023; 24(1): 1-4. ArticlePDF
- 3. Korean Statistical Information Service. Diabetes : ≥19 years, by sex [Internet]. Statistics Korea; 2024 [cited 2024 Apr 15]. Available from: https://kosis.kr/statHtml/statHtml.do?orgId=177&tblId=DT_11702_N102&conn_path=I2&language=en
- 4. Division of Health and Nutrition Survey and Analysis, Bureau of Chronic Disease Prevention and Control, Korea Disease Control and Prevention Agency. Diabetes awareness, treatment, and control, 2013-2021. Public Health Wkly Rep 2023; 16: 1521-1522.
- 5. Yun KO. Diabetes management through care communities. J Korean Diabetes 2016; 17(4): 271-276. ArticleLink
- 6. Graber AL, Christman BG, Alogna MT, Davidson JK. Evaluation of diabetes patient-education programs. Diabetes 1977; 26(1): 61-64. ArticlePubMed
- 7. Kang HJ. Current status and effects of nutrition education programs for diabetic patients in Korea. J Korean Diabetes 2018; 19(2): 106-112. ArticleLink
- 8. Song MS, Song KH, Ko SH, Ahn YB, Kim JS, Shin JH, et al. The long-term effect of a structured diabetes education program for uncontrolled type 2 diabetes mellitus patients-a 4-year follow-up. J Korean Diabetes Assoc 2005; 29(2): 140-150.
- 9. Shin KN, Lee HS, Kwon CS. Effects of nutrition education in type 2 diabetes mellitus on diabetes control and blood antioxidant status. J Korean Soc Food Sci Nutr 2011; 40(5): 689-695. Article
- 10. Song M. Diabetes self-management education in the community. J Korean Diabetes 2014; 15(2): 98-103. Article
- 11. Organization for Economic Cooperation and Development (OECD) iLibrary. Health at a glance 2023 [Internet]. OECD Publishing; 2023 [cited 2024 Apr 15]. Available from: https://www.oecd-ilibrary.org/content/publication/7a7afb35-en
- 12. Yun SK. Current status and problems of national diabetes care. J Korean Diabetes 2020; 21(4): 173-178. ArticlePDF
- 13. Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: translating evidence into action. Health Aff (Millwood) 2001; 20(6): 64-78. ArticlePubMed
- 14. Tsai AC, Morton SC, Mangione CM, Keeler EB. A meta-analysis of interventions to improve care for chronic illnesses. Am J Manag Care 2005; 11(8): 478-488. PubMedPMC
- 15. Lee YK. Challenges in the management of diabetes in primary care. J Korean Diabetes 2020; 21(3): 161-165. ArticlePDF
- 16. Kim HS, Yoo BN, Lee EW. Evaluation of the national chronic diseases management policy: performance and future directions. Public Health Aff 2018; 2(1): 105-120. ArticlePDF
- 17. Lee JR. Review the change of chronic disease care in Korea. J Korean Diabetes 2022; 23(4): 251-257. ArticlePDF
- 18. Song E, Kim YE, Ji S. Impact of a primary health care chronic diseases management pilot program. Korean J Med 2021; 96(1): 7-12. ArticlePDF
- 19. Kim JH, Chang SA. Effect of diabetes education program on glycemic control and self management for patients with type 2 diabetes mellitus. Diabetes Metab J 2009; 33(6): 518-525. Article
- 20. Lim HS, Chyun JH, Kim YS, Nam MS. Effect of nutrition education on diabetic management in diabetic patients. Korean J Nutr 2001; 34(1): 69-78.
- 21. Bae SY, Lee YH, Kim YH. An analysis on convergence of the efficiency and productivity change in Korean university hospitals. J Korea Serv Manag Soc 2009; 10(3): 53-95. Article
- 22. Joo J, Cho JJ, Kwon YJ, Lee Y, Shin DW. A qualitative study of satisfaction with the community-based primary care project among primary care patients and its efficacy. J Korean Med Assoc 2017; 60(2): 173-182. ArticleLink
- 23. Hwang JH, Choi YK, Lee YK, Yoon NH. Experience of community-based primary care patients in Korea: using focus group interview. Korean J Health Educ Promot 2020; 37(5): 51-67. Article
- 24. Kang HJ, Shin EM, Kim KW. Evaluation of nutrition education for diabetes mellitus management of older adults. Korean J Community Nutr 2009; 14(6): 734-745.
- 25. Jung JG, Chung EY, Kim AR, Park HJ, Kim YJ, Ban YH, et al. Improvement of knowledge, self-efficacy and self-care behaviors among diabetic patients participated in the education program of Sejong Center for Hypertension and Diabetes Management. J Agric Med Community Health 2017; 42(4): 234-243.
- 26. Chung J, Lee YK, Lee P. Development of nutrition-focused hypertension and diabetes education program for patients linked to clinics and public health centers. Korea Health Promotion Institute; 2020 Dec. Report No. 연구-04-2020-006-01.
- 27. Bijl JV, Poelgeest-Eeltink AV, Shortridge-Baggett L. The psychometric properties of the diabetes management self-efficacy scale for patients with type 2 diabetes mellitus. J Adv Nurs 1999; 30(2): 352-359. ArticlePubMedLink
- 28. Lee HJ, Lee JJ, Hwang TY, Kam S. Development and evaluation of a community staged education program for the cardiocerebrovascular disease high-risk patients. J Agric Med Community Health 2012; 37(3): 167-180. Article
- 29. Committee of Clinical Practice Guidelines, Korean Society for the Study of Obesity (KSSO). Evaluation and treatment of obesity and its comorbidities: 2022 update of clinical practice guidelines for obesity by the Korean Society for the Study of Obesity. J Obes Metab Syndr 2023; 32(1): 1-24. ArticlePubMedPMC
- 30. Oldridge NB, Stump TE, Nothwehr FK, Clark DO. Prevalence and outcomes of comorbid metabolic and cardiovascular conditions in middle- and older-age adults. J Clin Epidemiol 2001; 54(9): 928-934. ArticlePubMed
- 31. Funnell MM, Anderson RM. Empowerment and self-management of diabetes. Clin Diabetes 2004; 22(3): 123-127. ArticlePDF
- 32. Oh JY, Kim SB. Development and effects’ analysis of nutrition education program for diabetes mellitus at community health center - focused on individual daily energy requirements and food exchange units -. Korean J Community Nutr 2010; 15(4): 485-497.
- 33. Reaven GM. Compensatory hyperinsulinemia and the development of an atherogenic lipoprotein profile: the price paid to maintain glucose homeostasis in insulin-resistant individuals. Endocrinol Metab Clin North Am 2005; 34(1): 49-62. ArticlePubMed
- 34. Yeo SJ, Kim BH. Effects of an intensive management program for diabetic patients on a blood biochemical profile and diabetes knowledge. Korean J Community Nutr 2018; 23(2): 148-161. ArticleLink
- 35. Noh J. 2023 clinical practice guidelines for diabetes: recommendations for pharmacological treatment of type 2 diabetes. J Korean Diabetes 2023; 24(3): 127-134. ArticlePDF
- 36. Gillett MJ. International Expert Committee report on the role of the A1c assay in the diagnosis of diabetes: Diabetes Care 2009; 32(7): 1327-1334. Clin Biochem Rev 2009; 30(4): 197-200. PubMedPMC
- 37. Cheong W, Yim J, Oh D, Im JS, Ko KP, Kim Y. Effects of Chronic disease management based on clinics for blood pressure or glycemic control in patients with hypertension or type 2 diabetes mellitus. J Agric Med Community Health 2013; 38(2): 108-115. Article
- 38. Yuan C, Lai CW, Chan LW, Chow M, Law HK, Ying M. The effect of diabetes self-management education on body weight, glycemic control, and other metabolic markers in patients with type 2 diabetes mellitus. J Diabetes Res 2014; 2014: 789761.ArticlePubMedPMCPDF
- 39. Moon SH, Lee YW, Ham OK, Kim SH. The effect of the experience of diabetes education on knowledge, self-care behavior and glycosylated hemoglobin in type 2 diabetic patients. J Korean Acad Soc Nurs Educ 2014; 20(1): 81-92. Article
- 40. Song M, Choi S, Kim S, Seo K, Lee SJ, Kim EH. Development and validation of the diabetes management self-efficacy scale for older adults (DMSES-O). J Muscle Joint Health 2014; 21(3): 184-194. Article
- 41. Park JY, Ko IS. Development of a comprehensive self-management program promoting self efficacy for type 2 diabetic patients. J Korean Acad Fundam Nurs 2012; 19(1): 74-86. Article
- 42. Choi SY, Song MS. Behavior change theories in diabetes self-management: a conceptual review. Perspect Nurs Sci 2010; 7(1): 1-9.
- 43. Keum HS, Suh SR, Han S. The influence of self-management knowledge and distress on diabetes management self-efficacy in type 2 diabetes patients. J Korea Acad Ind Coop Soc 2020; 21(9): 498-508.
- 44. Bandura A. Self-efficacy mechanism in human agency. Am Psychol 1982; 37(2): 122-147. Article
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
Cite- Figure
-
- We recommend
- Related articles
-
- The impact of flash continuous glucose monitoring and nutrition coaching on dietary self-efficacy and weight management in university students in Korea: a pre-post intervention study
- Effects of a nutrition education program on metabolic syndrome risk factors in middle-aged Korean adults: an intervention study
Impact of a public health center nutrition education program on patients with type 2 diabetes in a primary care-based chronic disease management project: a pilot intervention study
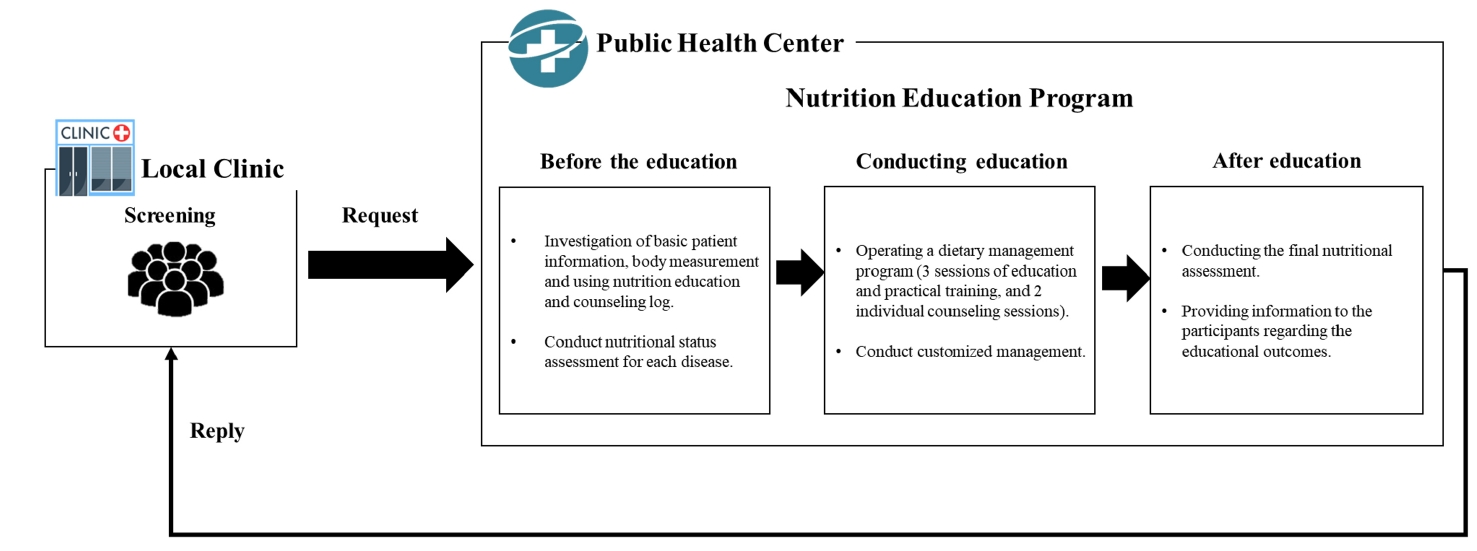
Fig. 1. Procedure for nutrition education program in collaboration between a clinic and public health center.
Fig. 1.
Impact of a public health center nutrition education program on patients with type 2 diabetes in a primary care-based chronic disease management project: a pilot intervention study
| Week | Section | Content | Method |
|---|---|---|---|
| 1 | Pre-assessment and evaluation | • Conducting a nutritional status assessment | Online |
| • Subject basic information and dietary habits survey, etc. | |||
| 2 | ① Customized management | • Guidance for the first session of nutritional education | Online |
| • Encouragement for participation, and the like | |||
| 3 |
1st basic nutrition education | • Implementation of basic education | Face to face |
| [The Basic principles of dietary management for diabetic patients] | |||
| - Diabetes mellitus etiology | |||
| - The significance of dietary therapy | |||
| - Diabetes and its complications | |||
| - Eating a balanced diet regularly | |||
| • Results of the first education and personalized management feedback | |||
| 4 | ② Customized management | • Guidance on the second session of nutritional education | Online |
| • Blood sugar check | |||
| 5 |
2nd in-depth nutrition education | • Conduct in-depth training | Face to face |
| [Blood glucose management in special circumstances] | |||
| - When sick, when exercising, and blood sugar management | |||
| - Symptoms and management of hypoglycemia | |||
| - Considerations for popular folk remedies, etc. | |||
| • Results feedback from the second session of education and personalized management | |||
| 6 | ③ Customized management | • Guidance on the third session of nutritional practicum education | Online |
| • Education content reminding | |||
| 7 |
3rd practical training |
• Guidance for the Third Session of nutritional practical training | Face to face |
| [Diabetes taste testing event] | |||
| - Portion control experiment with personal meal size | |||
| - Exploring adequate meal portions for myself | |||
| 8 | ④ Customized management | • Personal consultation guide | Online |
| • Blood sugar check | |||
| 9 | 4th individual consultation | • Conduct individual education and counseling | Online |
| • Results feedback from the fourth session of counseling and personalized management | |||
| 10 | ⑤ Customized management | • Counseling content reminding | Online |
| • Question and answer session | |||
| 11 | ⑥ Customized management | • Personal consultation guide | Online |
| • Blood sugar check | |||
| 12 | 5th individual consultation | • Conducting individual education and counseling | Online |
| • The end of the program | |||
| • Final management results feedback |
| Variable | Participant (n = 17) |
|---|---|
| Sex | |
| Male | 3 (17.6) |
| Female | 14 (82.4) |
| Age (year) | 62.71 ± 6.56 |
| 19–64 | 10 (58.8) |
| ≥ 65 | 7 (41.2) |
| Classification of obesity |
|
| Normal | 1 (5.9) |
| Overweight | 11 (64.7) |
| Obesity | 5 (29.4) |
| Variable | Participant (n = 17) |
P-value |
|
|---|---|---|---|
| Before | After | ||
| Weight (kg) | 63.5 ± 10.3 | 63.7 ± 10.8 | 0.918 |
| BMI (kg/m2) | 25.1 ± 2.3 | 25.1 ± 2.5 | 0.850 |
| Waist circumference (cm) | 88.3 ± 7.3 | 89.1 ± 8.1 | 0.582 |
| Body fat mass (kg) | 21.8 ± 5.8 | 21.0 ± 5.6 | 0.231 |
| Percent body fat (%) | 33.4 ± 3.9 | 33.1 ± 4.0 | 0.209 |
| Muscle mass (kg) | 38.4 ± 6.2 | 38.7 ± 6.4 | 0.378 |
| SBP (mm/Hg) | 117.7 ± 11.0 | 116.9 ± 13.5 | 0.850 |
| DBP (mm/Hg) | 71.2 ± 7.8 | 71.2 ± 19.0 | 0.314 |
| Variable | Participant (n = 17) |
P-value |
|
|---|---|---|---|
| Before | After | ||
| Fasting plasma glucose (mg/dL) | 123.1 ± 21.0 | 119.8 ± 23.3 | 0.981 |
| HbA1c (%) | 6.5 ± 0.5 | 6.4 ± 0.5 | 0.029 |
| Cholesterol | |||
| Total cholesterol (mg/dL) | 166.4 ± 49.7 | 151.9 ± 37.7 | 0.047 |
| LDL-cholesterol (mg/dL) | 82.6 ± 38.8 | 56.9 ± 22.4 | 0.014 |
| HDL-cholesterol (mg/dL) | 58.7 ± 16.3 | 61.1 ± 15.7 | 0.066 |
| Triglyceride (mg/dL) | 132.6 ± 64.4 | 175.6 ± 73.4 | 0.074 |
| Nutrition knowledge | Participant (n = 17) |
P-value |
|
|---|---|---|---|
| Before | After | ||
| Diabetes is caused by a deficiency or lack of insulin. | 7.7 ± 4.4 | 10.0 ± 0.0 | 0.046 |
| The medication is more crucial than diet or exercise in the treatment of diabetes. | 5.3 ± 5.1 | 9.4 ± 2.4 | 0.008 |
| If there are no specific symptoms, treatment may not be necessary for diabetes. | 8.2 ± 3.9 | 10.0 ± 0.0 | 0.083 |
| If blood sugar levels continue to rise, it can lead to visual impairment or impaired kidney function. | 10.0 ± 0.0 | 10.0 ± 0.0 | > 0.999 |
| If there is a high risk of low blood sugar, it is possible to consume a pre-exercise snack. | 10.0 ± 0.0 | 10.0 ± 0.0 | > 0.999 |
| After taking diabetes medication or receiving an insulin injection, if symptoms such as cold sweats, palpitations, hunger, fatigue, trembling hands, and headache occur, patients with diabetes should consume one tablespoon of sugar (15 g). | 9.4 ± 2.4 | 10.0 ± 0.0 | 0.317 |
| Maintaining a normal body weight is important for blood sugar control. | 10.0 ± 0.0 | 10.0 ± 0.0 | > 0.999 |
| Diabetic patients should not forego blood sugar monitoring and meals, as hypoglycemia may occur after alcohol consumption. | 7.7 ± 4.3 | 10.0 ± 0.0 | 0.046 |
| Fruits and vegetables contribute to lowering blood sugar levels. | 5.3 ± 5.1 | 7.1 ± 4.7 | 0.083 |
| Mixed grain rice can be consumed in larger quantities compared to white rice. | 7.1 ± 4.7 | 9.4 ± 2.4 | 0.046 |
| Nutritional knowledge total score | 80.6 ± 15.2 | 95.9 ± 6.2 | < 0.001 |
| Component | Participant (n = 17) |
P-value |
|
|---|---|---|---|
| Before | After | ||
| I can adhere to dietary practices for blood pressure and blood sugar control. | 3.9 ± 1.0 | 4.1 ± 0.8 | 0.157 |
| I can control the amount of meals and keep it constant. | 3.5 ± 0.8 | 4.2 ± 0.8 | 0.002 |
| I can visit the clinic regularly to check the condition of the disease and get a complication check. | 4.2 ± 0.7 | 4.4 ± 0.6 | 0.046 |
| I can maintain normal blood pressure and blood sugar levels. | 3.7 ± 0.9 | 4.1 ± 0.8 | 0.035 |
| I can keep my body weight constant. | 3.9 ± 0.7 | 3.9 ± 0.7 | > 0.999 |
| I can manage stress or anxiety just as effectively as during normal times. | 3.4 ± 0.8 | 3.8 ± 0.9 | 0.070 |
| I can ask my family for help when I have poor blood pressure/blood sugar control. | 3.5 ± 0.9 | 4.1 ± 0.7 | 0.015 |
| I can always practice eating blandly. | 3.8 ± 1.2 | 4.2 ± 0.9 | 0.023 |
| Self-efficacy total score | 29.7 ± 5.0 | 32.8 ± 5.2 | 0.002 |
Table 1. 12-Week dietary lifestyle management program for diabetes patients
The weeks indicate the “nutrition education program” included in the dietary management program.
Table 2. Baseline characteristics of patients
n (%) or Mean ± SD. Normal, 18.5 kg/m2–22.9 kg/m2; overweight, 23 kg/m2–24.9 kg/m2; obesity, > 25 kg/m2.
Table 3. Changes in anthropometric and body composition characteristics after diabetes education
Mean ± SD. BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure. Significance as determined by Wilcoxon’s signed-ranks test (
Table 4. Changes in blood biochemistry after diabetes education
Mean ± SD. HbA1c, hemoglobin A1c; LDL, low density lipoprotein; HDL, high density lipoprotein. Significance as determined by Wilcoxon’s signed-ranks test (
Table 5. Changes in nutrition knowledge questionnaire after diabetes education
Mean ± SD. Significance as determined by Wilcoxon’s signed-ranks test (
Table 6. Changes in self-efficacy after diabetes education
Mean ± SD. Significance as determined by Wilcoxon’s signed-ranks test (


