
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 30(1); 2025 > Article
-
Research Article
- Effects of a multi-component program based on partially hydrolyzed guar gum (Sunfiber®) on glycemic control in South Korea: a single-arm, pre-post comparison pilot clinical trial
-
Hyoung Su Park1)
 , A-Hyun Jeong2), Hyejung Hong3), Hana Jang4), Hye-Jin Kim5),†
, A-Hyun Jeong2), Hyejung Hong3), Hana Jang4), Hye-Jin Kim5),† -
Korean Journal of Community Nutrition 2025;30(1):40-52.
DOI: https://doi.org/10.5720/kjcn.2024.00276
Published online: February 28, 2025
1)Leader, R&D Group, Maeil Health Nutrition Co., Ltd, Pyeongtaek, Korea
2)Pro, R&D Group, Maeil Health Nutrition Co., Ltd, Pyeongtaek, Korea
3)Leader, Medical Food Division, Maeil Dairies Co., Ltd, Seoul, Korea
4)Pro, Medical Food Division, Maeil Dairies Co., Ltd, Seoul, Korea
5)Director, R&D Group, Maeil Health Nutrition Co., Ltd, Pyeongtaek, Korea
- †Corresponding author: Hye-Jin Kim R&D Group, Maeil Health Nutrition Co., Ltd, Pyeongtaek 17714, Korea Tel: +82-31-612-3935 Fax: +82-31-668-0247 Email: hyejink@maeil.com
• Received: November 18, 2024 • Revised: January 9, 2025 • Accepted: February 12, 2025
© 2025 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 10,047 Views
- 50 Download
- 2 Crossref
This article has been corrected. See "Erratum: Effects of a multi-component program based on partially hydrolyzed guar gum (Sunfiber®) on glycemic control in South Korea: a single-arm, pre-post comparison pilot clinical trial" in Volume 30 on page 173.
Abstract
-
Objectives
- The aim of this study was to assess the impact of a multi-component program, including partially hydrolyzed guar gum (PHGG, Sunfiber®) supplementation, on glycemic control, gut health, and nutritional status to support diabetes prevention and management among Korean adults.
-
Methods
- A single-arm trial was conducted with 29 adults (aged 20-55 years) with fasting plasma glucose (FPG) ≥ 100 mg/dL. Over a six-week period, participants engaged in a multi-component program that incorporated the supplementation of PHGG (Sunfiber®, 12.5 g/day), weekly nutritional coaching, and the use of continuous glucose monitoring devices. The program’s effectiveness was evaluated by measuring FPG and glycated hemoglobin (HbA1c) levels through blood tests conducted before and after the intervention. Improvements in gut health were gauged using the Korean Gut Quotient Measurement Scales, while enhancements in nutritional status were assessed using the Nutrition Quotient (NQ) and surveys that evaluated improvements in gut health and nutritional status.
-
Results
- Participants’ average age was 43.89 years, with approximately 80% being male. Most participants (about 75%) were classified as overweight or obese. After six-weeks, 17 participants who adhered closely to the program (meeting certification criteria) exhibited significant reductions in key blood glucose markers. FPG levels decreased from 113.06 ± 23.16 mg/dL to 106.24 ± 16.33 mg/dL (P < 0.05), and HbA1c levels decreased from 6.08% ± 0.81% to 5.87% ± 0.53% (P < 0.05). The NQ evaluation revealed significant increases in comprehensive nutrition scores, and in the balance and practice domain scores for all participants (P < 0.05). Furthermore, in the gut health survey, approximately 82.1% of all participants reported experiencing positive changes.
-
Conclusion
- Among adults with elevated FPG levels, a multi-component intervention program that included PHGG (Sunfiber®) supplementation, structured dietary management, and the use of health-monitoring devices showed significant benefits in improving glycemic control, overall nutritional status, and gut health.
-
Trial Registration
- Clinical Research Information Service Identifier: KCT0010049.
INTRODUCTION
METHODS
RESULTS
DISCUSSION
-
CONFLICT OF INTEREST
This study was conducted using Selex Sunfiber Guar gum Prebiotics (Sunfiber®) from Maeil Health Nutrition Co., Ltd. However, there are no financial or other issues that might lead to a conflict of interest.
-
FUNDING
None.
-
DATA AVAILABILITY
Research data is available upon request to the corresponding author.
NOTES
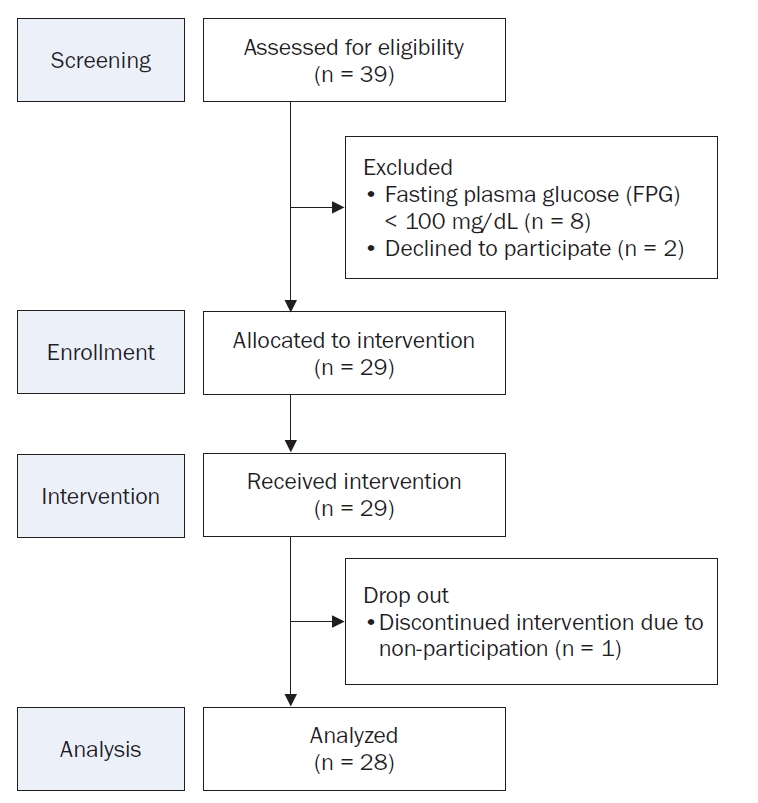
Fig. 2.Method for partially hydrolyzed guar gum (PHGG, Sunfiber®) supplementation and meal recording using the selex app.
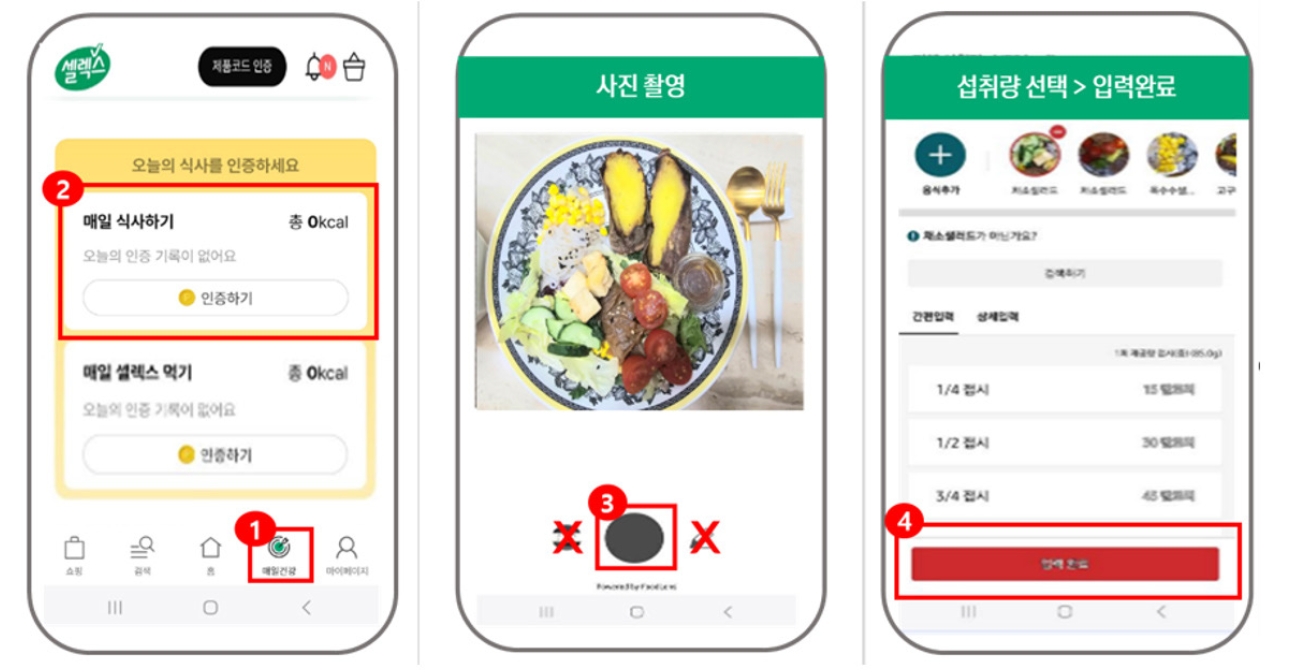
Fig. 3.
Changes in (A) fasting plasma glucose and (B) glycated hemoglobin levels in among all participants and by compliance status. Mean ± SD.
*Indicates a significant difference at P < 0.05. P-values were determined using a paired t-test or Wilcoxon’s signed-rank test, depending on normality.
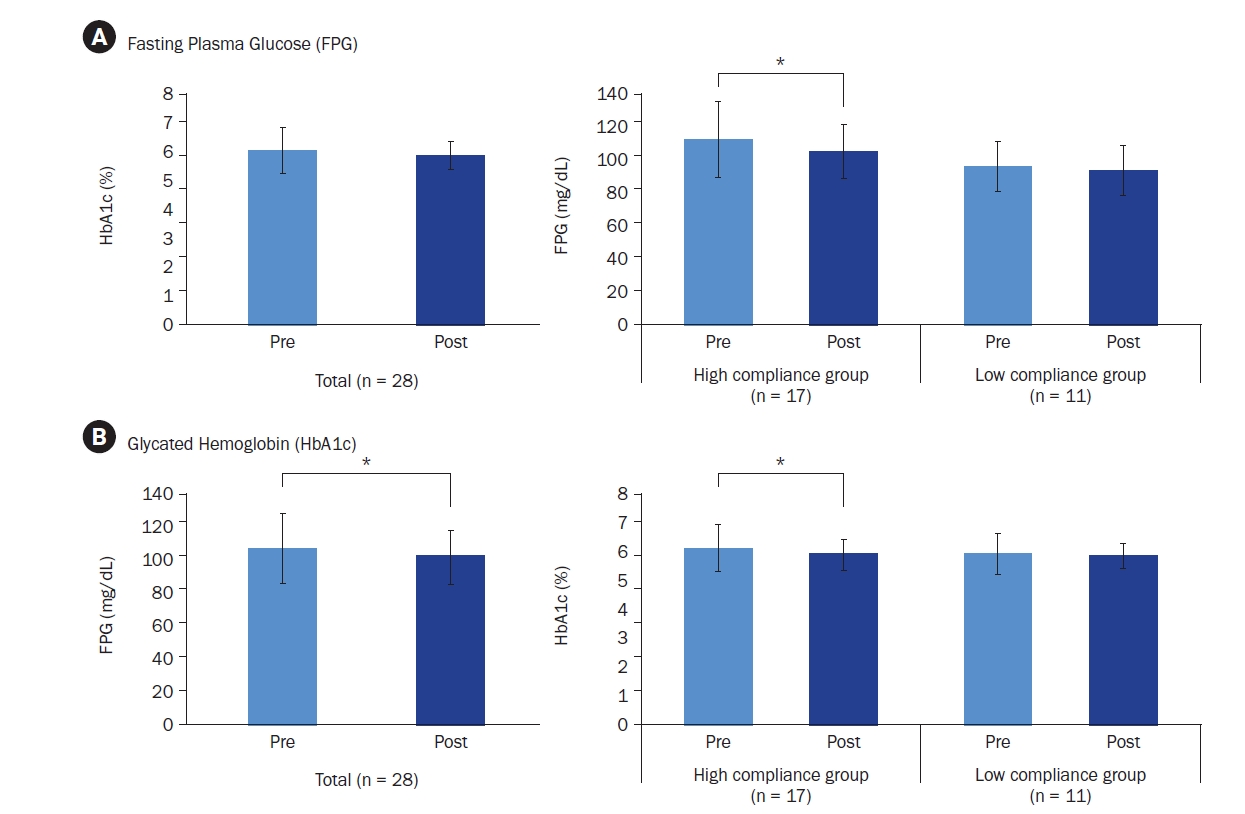
Fig. 4.
Changes in fasting plasma glucose (FPG) and glycated hemoglobin (HbA1c) levels in (A) male and (B) female participants. Mean ± SD.
*Indicates a significant difference at P < 0.05. P-values were determined using a paired t-test or Wilcoxon’s signed-rank test, depending on normality.
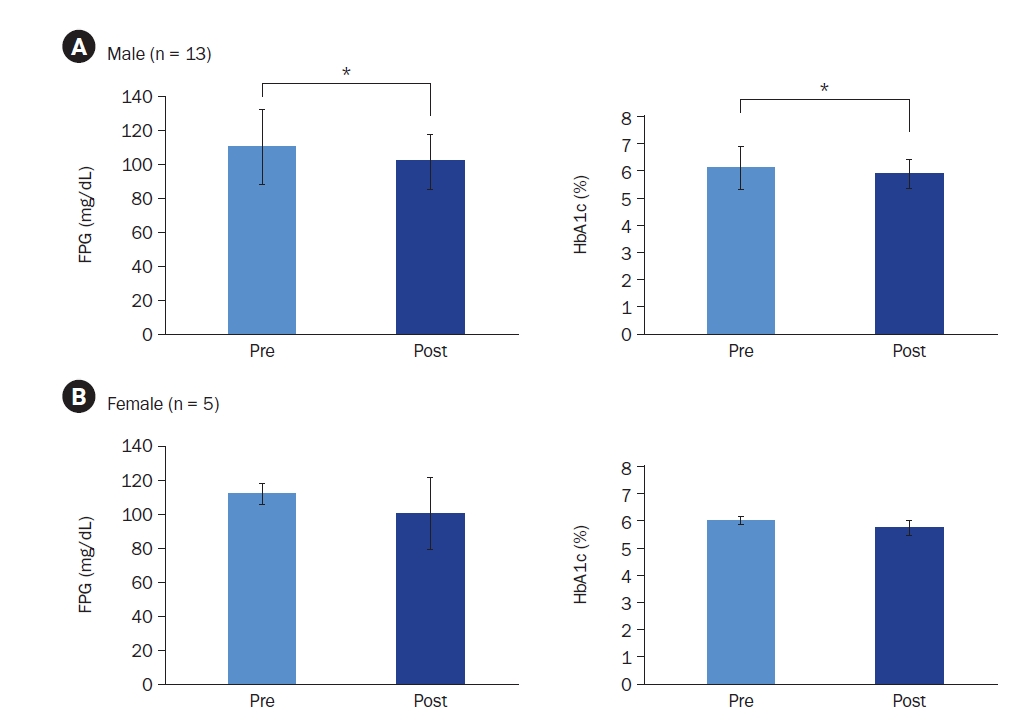
Fig. 5.
Changes in nutrition scores based on nutrition quotient (NQ) assessment: balance, moderation, practice, and nutrition quotient (n = 28). Mean ± SD.
*Indicates a significant difference at P < 0.05 and **indicates a significant difference at P < 0.01. P-values were determined using a paired t-test or Wilcoxon’s signed-rank test, depending on normality.
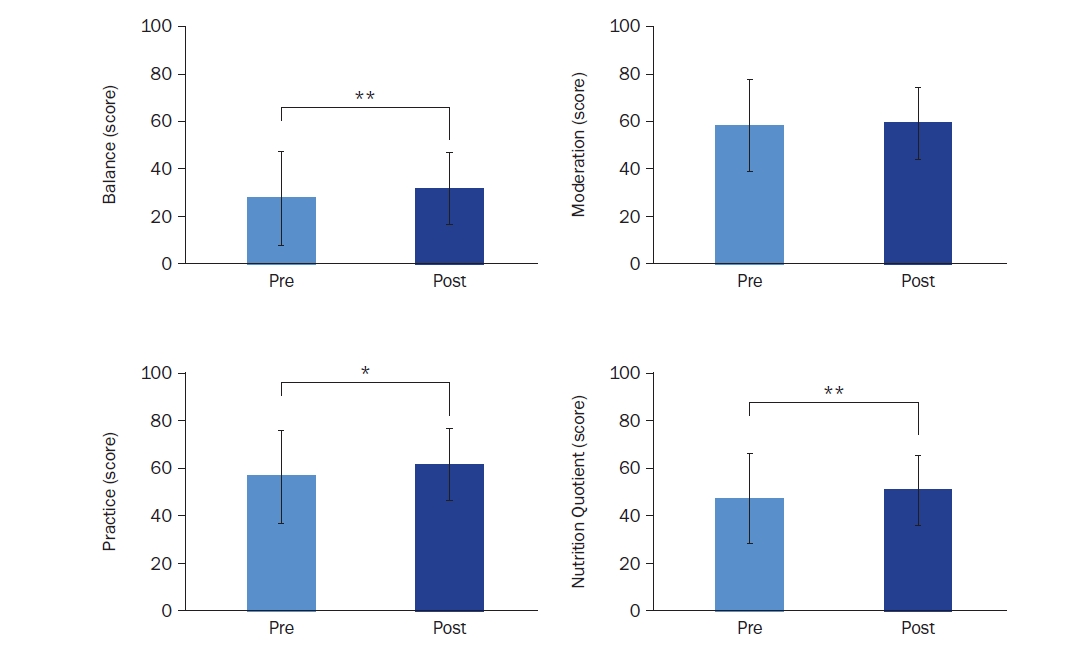
Table 1.Baseline characteristics of study participants
Table 2.Changes in gut health and bowel movement characteristics before and after the program
Table 3.Assessment of gut health status changes among participants post-program
Table 4.Participant satisfaction with overall program
| Category | Subject (n = 28) |
|---|---|
| Overall program satisfaction | |
| Very satisfied | 13 (46.4) |
| Satisfied | 12 (42.9) |
| Neutral | 3 (10.7) |
| Dissatisfied | 0 (0.0) |
| Very dissatisfied | 0 (0.0) |
Table 5.Evaluation of participant perceptions on the effectiveness of interventions for blood glucose and gut health management
- 1. Lee SK, Shin DH, Kim YH, Lee KS. Effect of diabetes education through pattern management on self-care and self-efficacy in patients with type 2 diabetes. Int J Environ Res Public Health 2019; 16(18): 3323.ArticlePubMedPMC
- 2. Korean Diabetes Association (KDA). Diabetes Fact Sheet in Korea 2024. KDA; 2024. p. 1-71.
- 3. National Health Information Potal. Diabetes [Internet]. Korea Disease Control and Prevention Agency; 2020 [updated 2024 Sep 9; cited 2024 Nov 15]. Available from: https://health.kdca.go.kr/healthinfo/biz/health/gnrlzHealthInfo/gnrlzHealthInfo/gnrlzHealthInfoView.do?cntnts_sn=5305
- 4. Kwon HS. Prevalence and treatment status of diabetes mellitus in Korea. J Korean Med Assoc 2023; 66(7): 404-407. ArticlePDF
- 5. Weickert MO, Pfeiffer AF. Metabolic effects of dietary fiber consumption and prevention of diabetes. J Nutr 2008; 138(3): 439-442. ArticlePubMed
- 6. Post RE, Mainous AG 3rd, King DE, Simpson KN. Dietary fiber for the treatment of type 2 diabetes mellitus: a meta-analysis. J Am Board Fam Med 2012; 25(1): 16-23. Article
- 7. Chandalia M, Garg A, Lutjohann D, von Bergmann K, Grundy SM, Brinkley LJ. Beneficial effects of high dietary fiber intake in patients with type 2 diabetes mellitus. N Engl J Med 2000; 342(19): 1392-1398. ArticlePubMed
- 8. Lattimer JM, Haub MD. Effects of dietary fiber and its components on metabolic health. Nutrients 2010; 2(12): 1266-1289. ArticlePubMedPMC
- 9. Sami W, Ansari T, Butt NS, Hamid MRA. Effect of diet on type 2 diabetes mellitus: a review. Int J Health Sci (Qassim) 2017; 11(2): 65-71.
- 10. Lyu YS, Kim JH, Kim SY. Gut microbiota and diabetes. J Korean Diabetes 2024; 25(3): 117-123. ArticlePDF
- 11. Holscher HD. Dietary fiber and prebiotics and the gastrointestinal microbiota. Gut Microbes 2017; 8(2): 172-184. ArticlePubMedPMCLink
- 12. Chen M, Yang R, Wang Y, Jia Y, Liu J, Wang G. Non-linear associations of body mass index with impaired fasting glucose, β-cell dysfunction, and insulin resistance in nondiabetic Chinese individuals: a cross-sectional study. Endokrynol Pol 2021; 72(6): 618-624. ArticlePubMed
- 13. Rhee SY, Chon S, Ahn KJ, Woo JT; Korean Diabetes Prevention Study Investigators. Hospital-based Korean Diabetes prevention study: a prospective, multi-center, randomized, open-label controlled study. Diabetes Metab J 2019; 43(1): 49-58. ArticlePubMedLink
- 14. Menezes MC, Duarte CK, Costa DVP, Lopes MS, Freitas PP, Campos SF, et al. A systematic review of effects, potentialities, and limitations of nutritional interventions aimed at managing obesity in primary and secondary health care. Nutrition 2020; 75-76: 110784.ArticlePubMed
- 15. Saslow LR, Mason AE, Kim S, Goldman V, Ploutz-Snyder R, Bayandorian H, et al. An online intervention comparing a very low-carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: a randomized controlled trial. J Med Internet Res 2017; 19(2): e36.ArticlePubMedPMC
- 16. Kim MS, Ryu JM, Kang M, Park J, Ahn YC, Kim YS. Development and adaptability of smartphone-based dietary coaching program for patients undergoing diabetes and prediabetes with continuous glucose monitoring device. J Health Info Stat 2023; 48(1): 36-50. ArticlePDF
- 17. Shreck E, Gonzalez JS, Cohen HW, Walker EA. Risk perception and self-management in urban, diverse adults with type 2 diabetes: the improving diabetes outcomes study. Int J Behav Med 2014; 21(1): 88-98. ArticlePubMedPMCPDF
- 18. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for adults with type 2 diabetes mellitus: a systematic review of the effect on glycemic control. Patient Educ Couns 2016; 99(6): 926-943. ArticlePubMed
- 19. Yuan C, Lai CW, Chan LW, Chow M, Law HK, Ying M. The effect of diabetes self-management education on body weight, glycemic control, and other metabolic markers in patients with type 2 diabetes mellitus. J Diabetes Res 2014; 2014: 789761.ArticlePubMedPMCPDF
- 20. Kim Y, Park JE, Lee BW, Jung CH, Park DA. Comparative effectiveness of telemonitoring versus usual care for type 2 diabetes: a systematic review and meta-analysis. J Telemed Telecare 2019; 25(10): 587-601. ArticlePubMedLink
- 21. Jiang Y, Ramachandran HJ, Teo JYC, Leong FL, Lim ST, Nguyen HD, et al. Effectiveness of a nurse-led smartphone-based self-management programme for people with poorly controlled type 2 diabetes: a randomized controlled trial. J Adv Nurs 2022; 78(4): 1154-1165. ArticlePubMed
- 22. Korean Diabetes Association (KDA). 2023 Clinical Practice Guidelines for Diabetes [Internet]. KDA; 2023 [cited 2025 Jan 8]. Available from: https://diabetes.or.kr/bbs/?code=guide&mode=view&number=1284&page=1&code=guide
- 23. Ministry of Food and Drug Safety. Ingredient-specific information for health functional foods [Internet]. Food Safety Korea; 2015 [cited 2024 Nov 14]. Available from: http://www.foodsafetykorea.go.kr/
- 24. Yook SM, Lim YS, Lee JS, Kim KN, Hwang HJ, Kwon S, et al. Revision of nutrition quotient for Korean adults: NQ-2021. J Nutr Health 2022; 55(2): 278-295. ArticleLink
- 25. Choi YJ, Cho JH, Lee DH, Song DJ, Kwon YJ, Baek SM, et al. Development of Koreans gut quotient measurement scales. Korean J Gastroenterol 2019; 73(6): 341-349. ArticlePubMedLink
- 26. Wolever TM. Relationship between dietary fiber content and composition in foods and the glycemic index. Am J Clin Nutr 1990; 51(1): 72-75. ArticlePubMed
- 27. Nishimune T, Yakushiji T, Sumimoto T, Taguchi S, Konishi Y, Nakahara S, et al. Glycemic response and fiber content of some foods. Am J Clin Nutr 1991; 54(2): 414-419. ArticlePubMed
- 28. Lee C, Shin JS. Effects of different fiber content of rice on blood glucose and triglyceride levels in normal subject. J Korean Soc Food Sci Nutr 2002; 31(6): 1048-1051. Article
- 29. Lairon D, Arnault N, Bertrais S, Planells R, Clero E, Hercberg S, et al. Dietary fiber intake and risk factors for cardiovascular disease in French adults. Am J Clin Nutr 2005; 82(6): 1185-1194. ArticlePubMed
- 30. Oh K, Hu FB, Cho E, Rexrode KM, Stampfer MJ, Manson JE, et al. Carbohydrate intake, glycemic index, glycemic load, and dietary fiber in relation to risk of stroke in women. Am J Epidemiol 2005; 161(2): 161-169. ArticlePubMed
- 31. Lee YS, Lee SY. The association between dietary fiber intake and prevalence of metabolic syndrome in middle-aged adults in Gyeonggi province. Korean J Health Promot 2015; 15(2): 75-82. Article
- 32. National Health Information Potal. Dietary nutrition [Internet]. Korea Disease Control and Prevention Agency; 2020 [updated 2024 Dec 26; cited 2024 Dec 30]. Available from: https://health.kdca.go.kr/healthinfo/biz/health/gnrlzHealthInfo/gnrlzHealthInfo/gnrlzHealthInfoView.do?cntnts_sn=5298
- 33. Yu KH, Chung CE, Cho SS, Ly SY. Analysis of dietary fiber intake in the Korean adult population using 2001 Korean National Health and Nutrition Survey data and newly established dietary fiber database. Korean J Nutr 2008; 41(1): 100-110.
- 34. Lim S, Shin H, Song JH, Kwak SH, Kang SM, Yoon JW, et al. Increasing prevalence of metabolic syndrome in Korea: the Korean National Health and Nutrition Examination Survey for 1998-2007. Diabetes Care 2011; 34(6): 1323-1328. ArticlePubMedPMC
- 35. Vuorinen-Markkola H, Sinisalo M, Koivisto VA. Guar gum in insulin-dependent diabetes: effects on glycemic control and serum lipoproteins. Am J Clin Nutr 1992; 56(6): 1056-1060. ArticlePubMed
- 36. Landin K, Holm G, Tengborn L, Smith U. Guar gum improves insulin sensitivity, blood lipids, blood pressure, and fibrinolysis in healthy men. Am J Clin Nutr 1992; 56(6): 1061-1065. ArticlePubMed
- 37. Taylor PJ, Thompson CH, Brinkworth GD. Effectiveness and acceptability of continuous glucose monitoring for type 2 diabetes management: a narrative review. J Diabetes Investig 2018; 9(4): 713-725. ArticlePubMedPMCLink
- 38. Nelson LA, Wallston KA, Kripalani S, Greevy RA Jr, Elasy TA, Bergner EM, et al. Mobile phone support for diabetes self-care among diverse adults: protocol for a three-arm randomized controlled trial. JMIR Res Protoc 2018; 7(4): e92. ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Comparative analysis of dietary and lifestyle habits according to the prediabetic status in young adults
Joungyoon Seo, SeongHee Shin, Yuri Kim, Yoo Kyoung Park
Journal of Nutrition and Health.2025; 58(5): 468. CrossRef - Partially Hydrolyzed Guar Gum Combined with a Low-Fat Diet Ameliorates Type 2 Diabetes Mellitus via Modulating Gut Microbiota and Fecal Metabolites
Zhiqiang Cao, Hongxia Li, Quantao Cai, Li Chen, Liangzhong Liu, Yuhan Tang, Zhe Zhu, Ping Yao
Nutrients.2025; 17(23): 3746. CrossRef
 Cite
CiteEffects of a multi-component program based on partially hydrolyzed guar gum (Sunfiber®) on glycemic control in South Korea: a single-arm, pre-post comparison pilot clinical trial
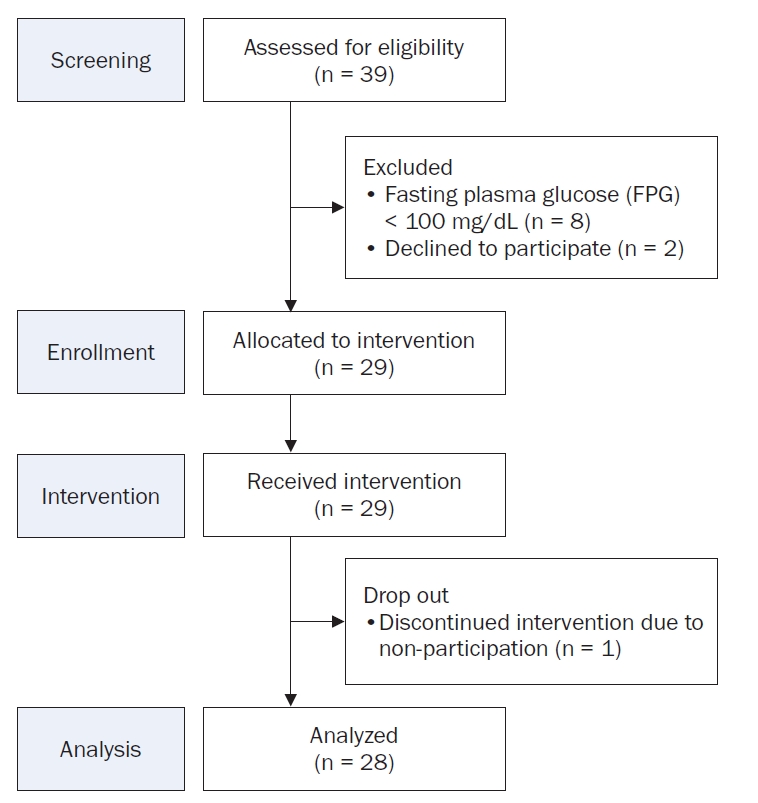
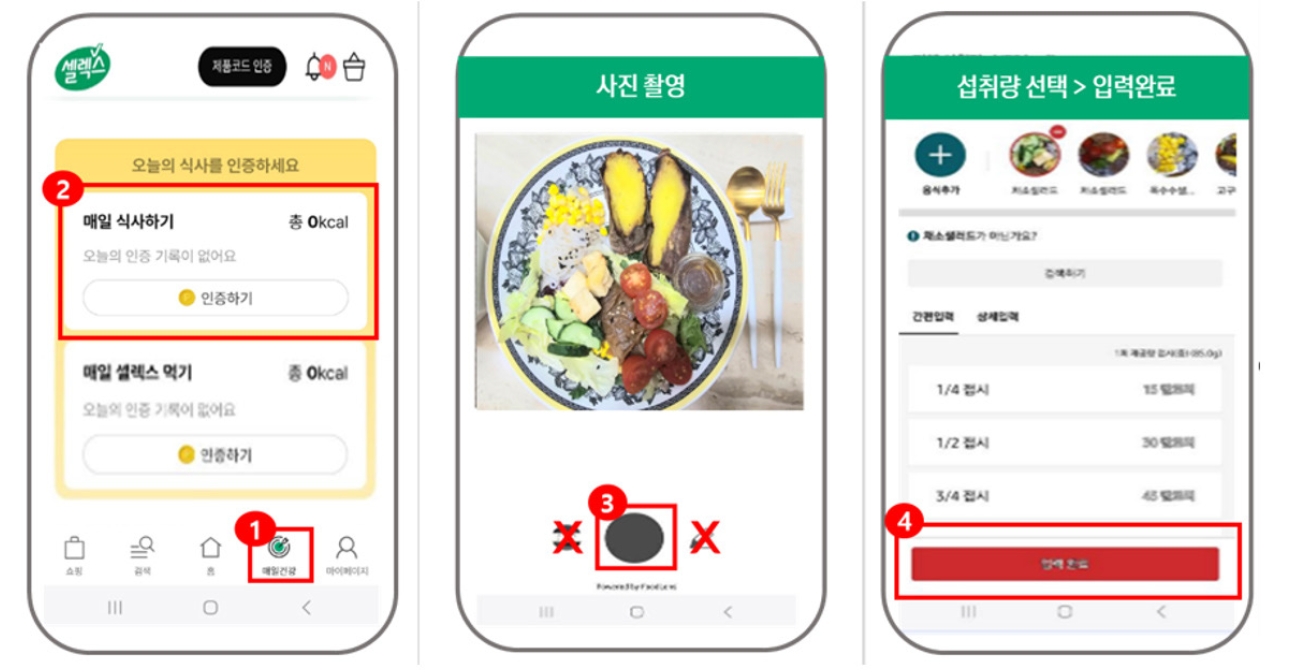
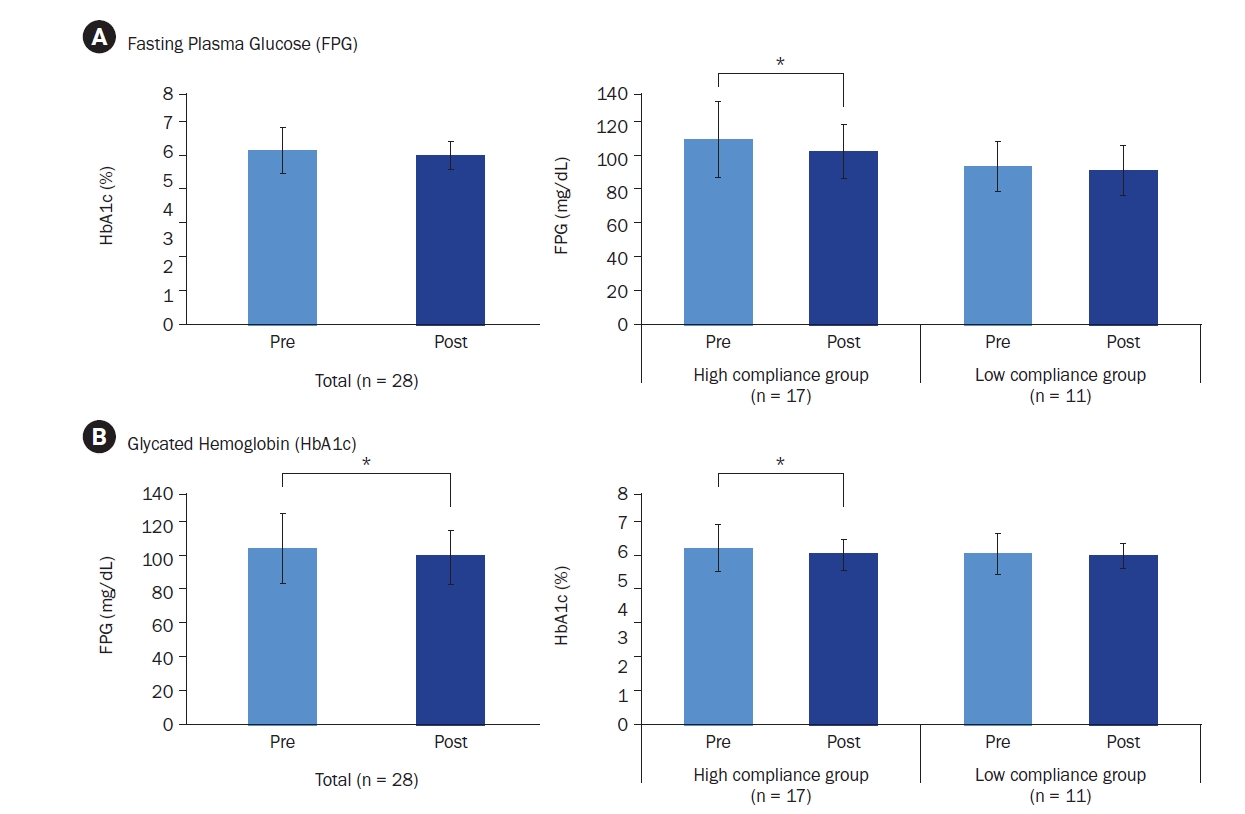
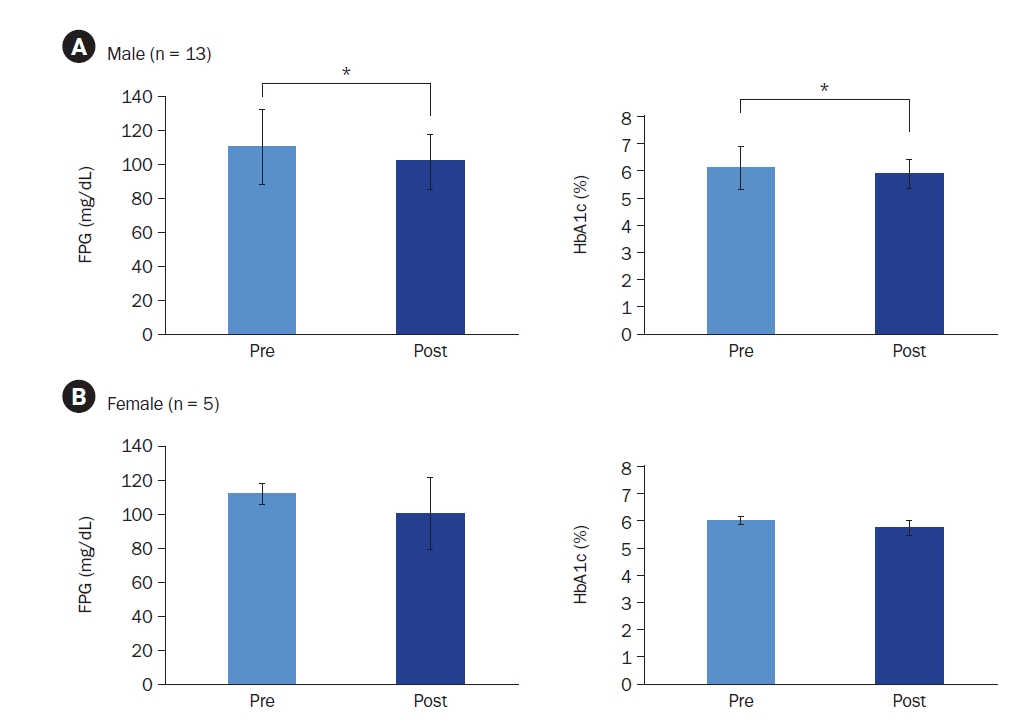
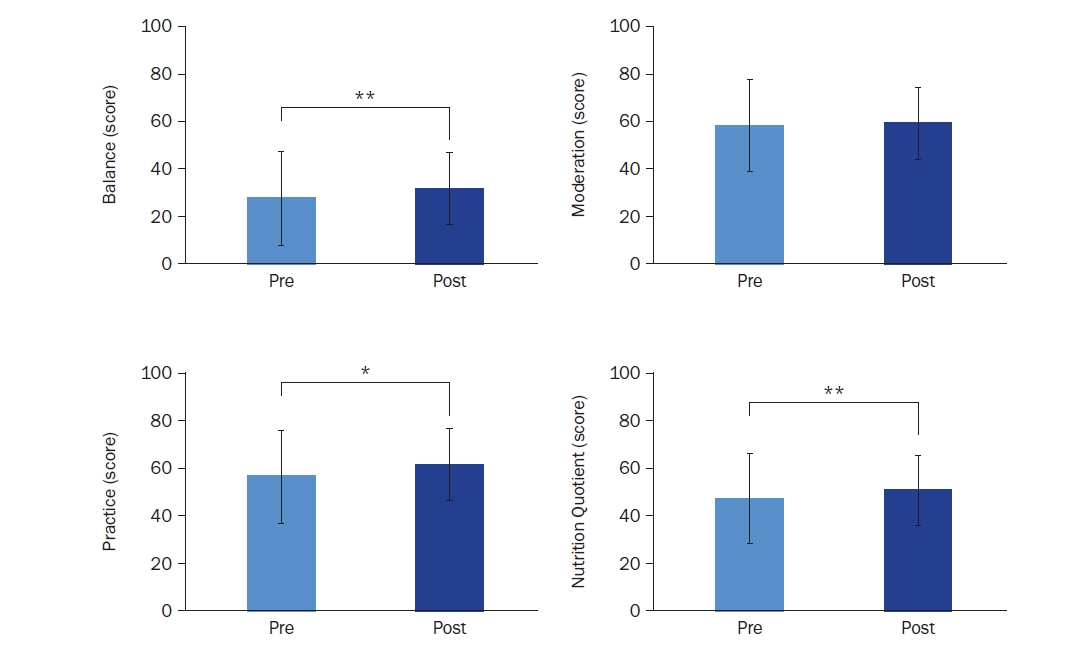
Fig. 1. Participant flowchart for the single-arm trial.
Fig. 2. Method for partially hydrolyzed guar gum (PHGG, Sunfiber®) supplementation and meal recording using the selex app.
Fig. 3. Changes in (A) fasting plasma glucose and (B) glycated hemoglobin levels in among all participants and by compliance status. Mean ± SD.*Indicates a significant difference at P < 0.05. P-values were determined using a paired t-test or Wilcoxon’s signed-rank test, depending on normality.
Fig. 4. Changes in fasting plasma glucose (FPG) and glycated hemoglobin (HbA1c) levels in (A) male and (B) female participants. Mean ± SD.*Indicates a significant difference at P < 0.05. P-values were determined using a paired t-test or Wilcoxon’s signed-rank test, depending on normality.
Fig. 5. Changes in nutrition scores based on nutrition quotient (NQ) assessment: balance, moderation, practice, and nutrition quotient (n = 28). Mean ± SD.*Indicates a significant difference at P < 0.05 and **indicates a significant difference at P < 0.01. P-values were determined using a paired t-test or Wilcoxon’s signed-rank test, depending on normality.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Effects of a multi-component program based on partially hydrolyzed guar gum (Sunfiber®) on glycemic control in South Korea: a single-arm, pre-post comparison pilot clinical trial
| Variable | Subject (n = 28) |
|---|---|
| Sex | |
| Male | 23 (82.1) |
| Female | 5 (17.9) |
| Age group (year) | |
| 20–29 | 1 (3.6) |
| 30–39 | 5 (17.9) |
| 40–49 | 16 (57.1) |
| 50–55 | 6 (21.4) |
| Body mass index | |
| Underweight | 0 (0.0) |
| Normal weight | 7 (25.0) |
| Overweight | 4 (14.3) |
| Obese | 17 (60.7) |
| Diabetes status | |
| Diabetes present | 6 (21.4) |
| Diabetes absent | 22 (78.6) |
| Intake of health functional food for blood glucose control | |
| Yes | 4 (14.3) |
| No | 24 (85.7) |
| Medication type (multiple responses allowed) | |
| Antihypertensive agents | 8 (28.6) |
| Lipid-lowering agents | 7 (25.0) |
| Antidiabetic agents | 2 (7.1) |
| Cholesterol-lowering agents | 1 (3.6) |
| Alopecia treatment agents | 1 (3.6) |
| Thyroid disorder medications | 1 (3.6) |
| Benign prostatic hyperplasia medications | 1 (3.6) |
| Category | Pre (n = 28) | Post (n = 28) | x2 | P-value |
|---|---|---|---|---|
| Gut health condition | ||||
| No issues | 9 (32.1) | 12 (42.9) | - | - |
| Mild issues | 11 (39.3) | 14 (50.0) | ||
| Severe issues | 8 (28.6) | 2 (7.1) | ||
| Stool consistency | ||||
| Pellet-like, very hard | 1 (3.6) | 1 (3.6) | - | - |
| Hard pellets but forms a lump | 1 (3.6) | 0 (0.0) | ||
| Like a sausage with cracks on the surface | 7 (25.0) | 4 (14.3) | ||
| Like a smooth and soft sausage | 9 (32.1) | 11 (39.3) | ||
| Soft, lumpy pieces | 7 (25.0) | 9 (32.1) | ||
| Mushy, scattered in the toilet bowl | 2 (7.1) | 3 (10.7) | ||
| Watery | 1 (3.6) | 0 (0.0) | ||
| Defecation frequency | ||||
| Daily | 17 (60.7) | 14 (50.0) | 2.80 | 0.423 |
| 5–6 times/week | 5 (17.9) | 9 (32.1) | ||
| 3–4 times/week | 6 (21.4) | 5 (17.9) | ||
| 1–2 times/week | 0 (0.0) | 0 (0.0) | ||
| Less than 3 times/month | 0 (0.0) | 0 (0.0) | ||
| Time spent on defecation | ||||
| Immediately | 4 (14.3) | 3 (10.7) | 4.533 | 0.475 |
| Within 5 minutes | 12 (42.9) | 13 (46.4) | ||
| 5–10 minutes | 6 (21.4) | 9 (32.1) | ||
| 10–15 minutes | 3 (10.7) | 1 (3.6) | ||
| 15–30 minutes | 3 (10.7) | 2 (7.1) | ||
| More than 30 minutes | 0 (0.0) | 0 (0.0) | ||
| Stool volume | ||||
| Less than 1 cup | 4 (14.3) | 1 (3.6) | - | - |
| 1–2 cups | 16 (57.1) | 21 (75.0) | ||
| 2–3 cups | 7 (25.0) | 5 (17.9) | ||
| 3–4 cups | 0 (0.0) | 1 (3.6) | ||
| More than 5 cups | 1 (3.6) | 0 (0.0) | ||
| Unknown due to watery stool | 0 (0.0) | 0 (0.0) |
| Category | Subject (n = 28) |
|---|---|
| Gut health change | |
| Significantly worsened | 0 (0.0) |
| Worsened | 0 (0.0) |
| Slightly worsened | 2 (7.1) |
| No change | 3 (10.7) |
| Slightly improved | 14 (50.0) |
| Improved | 6 (21.4) |
| Significantly improved | 3 (10.7) |
| Category | Subject (n = 28) |
|---|---|
| Overall program satisfaction | |
| Very satisfied | 13 (46.4) |
| Satisfied | 12 (42.9) |
| Neutral | 3 (10.7) |
| Dissatisfied | 0 (0.0) |
| Very dissatisfied | 0 (0.0) |
| Questions | Subject (n = 28) |
|---|---|
| Do you think that consuming ‘Selex Sunfiber Guar gum Prebiotics (Sunfiber®)’ helped with blood glucose management? | |
| Strongly agree | 4 (14.3) |
| Agree | 15 (53.6) |
| Neutral | 7 (25.0) |
| Disagree | 2 (7.1) |
| Strongly disagree | 0 (0.0) |
| Do you think that nutritional coaching on dietary intake was helpful for blood glucose management? | |
| Strongly agree | 9 (32.1) |
| Agree | 15 (53.6) |
| Neutral | 4 (14.3) |
| Disagree | 0 (0.0) |
| Strongly disagree | 0 (0.0) |
| Do you think that the use of continuous glucose monitoring was helpful for blood glucose management? | |
| Strongly agree | 15 (53.6) |
| Agree | 13 (46.4) |
| Neutral | 0 (0.0) |
| Disagree | 0 (0.0) |
| Strongly disagree | 0 (0.0) |
| Do you think that consuming ‘Selex Sunfiber Guar gum Prebiotics (Sunfiber®)’ contributed to gut health improvement? | |
| Strongly agree | 9 (32.1) |
| Agree | 13 (46.4) |
| Neutral | 6 (21.4) |
| Disagree | 0 (0.0) |
| Strongly disagree | 0 (0.0) |
Table 1. Baseline characteristics of study participants
n (%).
Table 2. Changes in gut health and bowel movement characteristics before and after the program
n (%).
Table 3. Assessment of gut health status changes among participants post-program
n (%).
Table 4. Participant satisfaction with overall program
n (%).
Table 5. Evaluation of participant perceptions on the effectiveness of interventions for blood glucose and gut health management
n (%).


