
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 30(5); 2025 > Article
-
Research Article
장애인대상 영양상담매뉴얼 개발 연구 -
이경민1),2)
 , 김우정3), 김소영4), 박영미5), 윤화영6), 전민선2),7),†
, 김우정3), 김소영4), 박영미5), 윤화영6), 전민선2),7),† - A study on the development of nutrition counseling manual and curriculum for the disabled in Korea: a mixed-methods study
-
Kyoung-Min Lee1),2), Woo-jeong Kim3), So-young Kim4), Young-mi Park5), Hwa-young Yoon6), Min-Sun Jeon2),7),†
-
Korean Journal of Community Nutrition 2025;30(5):376-388.
DOI: https://doi.org/10.5720/kjcn.2025.00192
Published online: October 31, 2025
1)충남대학교 식품영양학과 및 글로컬라이프케어 융합전공 박사과정생
2)충남대학교 글로컬라이프케어 혁신인재교육단
3)세브란스병원 영양팀장
4)국립암센터 부속병원 임상영양실장
5)분당서울대학교병원 영양실장
6)보바스기념병원 임상영양팀장
7)충남대학교 식품영양학과 교수
1)Ph.D. Student, Department of Food and Nutrition•Major of Glocal Life-Care Convergence, Chungnam National University, Daejeon, Korea
2)Interdisciplinary Education Center for the Innovative Next Generation Leaders in Glocal Lifecare, Chungnam National University, Daejeon, Korea
3)Head, Department of Clinical Nutrition, Severance Hospital, Yonsei University Health System, Seoul, Korea
4)Head, Department of Clinical Nutrition, National Cancer Center Hospital, Goyang, Korea
5)Head, Department of Clinical Nutrition, Seoul National University Bundang Hospital (SNUBH), Seongnam, Korea
6)Head, Department of Clinical Nutrition, Bobath Memorial Hospital, Seongnam, Korea
7)Professor, Department of Food and Nutrition, Chungnam National University, Daejeon, Korea
- †Corresponding author: Min-Sun Jeon Department of Food and Nutrition, Chungnam National University, 99 Daehak-ro, Yuseong-gu, Daejeon 34134, Korea Tel: +82-42-821-6836 Fax: +82-42-821-3335 Email: dearms@cnu.ac.kr
• Received: July 14, 2025 • Revised: August 20, 2025 • Accepted: September 30, 2025
© 2025 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 722 Views
- 32 Download
Abstract
-
Objectives
- Individuals with disabilities require targeted interventions to ameliorate disability-related conditions and improve overall health status. Nutritional challenges and counseling needs vary according to the type of disability, necessitating comprehensive assessments of dietary habits, physical activity, and food intake. Compared to traditional education, nutrition counseling offers a more sustainable and environmentally adaptable approach that effectively addresses individualized nutritional issues. Therefore, this study aimed to develop and evaluate a practical nutrition counseling manual and meal guidelines for people with disabilities in Korea, addressing their diverse dietary needs and improving nutritional care in social welfare facilities.
-
Methods
- A four-stage integrated research design was employed. Stage 1 involved qualitative research through in-depth interviews with 11 facility staff. In Stage 2, a nationwide survey (n = 249) was conducted based on the results of the interviews. Stage 3 integrated both qualitative and quantitative findings. Stage 4 focused on developing and evaluating a nutrition counseling manual and five types of meal guidelines through feedback from 26 nutritionists at 24 Korean Centers for Social Welfare Foodservice Management.
-
Results
- Six major nutrition counseling topics were identified: healthy eating, managing salt and sugar intake, dysphagia diet, appropriate intake, and hygiene. The manual and guidelines demonstrated high field usability, with average satisfaction scores of 3.98 ± 0.80, respectively.
-
Conclusion
- The integrated study resulted in the development of a specialized nutrition counseling manual and handbook for individuals with disabilities in Korean social welfare facilities. The materials were revised and improved based on practical evaluations by dietitians, enhancing their field applicability. These tools are expected to contribute to better dietary management and health promotion among facility residents. The developed materials reflect the real-world needs of people with disabilities and offer practical tools for effective nutrition counseling and dietary management in institutional settings.
INTRODUCTION
METHODS
1) 장애인 사회복지시설 종사자 대상 심층면접(1:1 in-depth interview)
(1) 연구 대상자 선정
(2) 심층면접 진행 방법
(3) 심층면접 내용 분석
2) 장애인 사회복지시설 종사자 대상 설문조사
(1) 연구 대상 시설 선정
(2) 설문지 구성 및 분석
1) 영양상담매뉴얼 개발
2) 영양상담매뉴얼 활용성 평가
RESULTS
1) 일반적 특성
2) 장애인 사회복지시설 종사자 대상 영양상담 주제 요구도
(1) 교육주제의 다양화
(2) 식사 흥미 유도 및 식사 지원 교육
(3) 기초적인 영양소 교육 및 기본 조리 교육
(4) 식품 알레르기 관리 방법
3) 장애인 사회복지시설 종사자 대상 영양상담 매체 요구도
(1) 시설 종사자 편의를 고려한 맞춤형 자료
(2) 온라인 및 오프라인의 교육 자료
1) 장애인 사회복지시설의 일반적 특성 및 입소•이용자 현황
2) 장애인 사회복지시설 영양상담 운영 현황
3) 장애인 사회복지시설 영양상담에 대한 인식
4) 장애인 사회복지시설 영양교육 주제 요구도
1) 장애인 사회복지시설 맞춤형 영양상담 내용 도출
2) 장애인 사회복지시설 맞춤형 영양상담매뉴얼 활용성 평가 결과
3) 맞춤형 영양상담매뉴얼 최종 개발
DISCUSSION
-
CONFLICT OF INTEREST
There are no financial or other issues that might lead to conflict of interest.
-
FUNDING
This research was supported by a grant from Ministry of Food and Drug Safety in 2022 (Grant No. 22192MFDS067).
-
DATA AVAILABILITY
Research data is available upon request to the corresponding author.
NOTES
Fig. 1.Analytical stages of mixed methods research integrating qualitative and quantitative approaches.
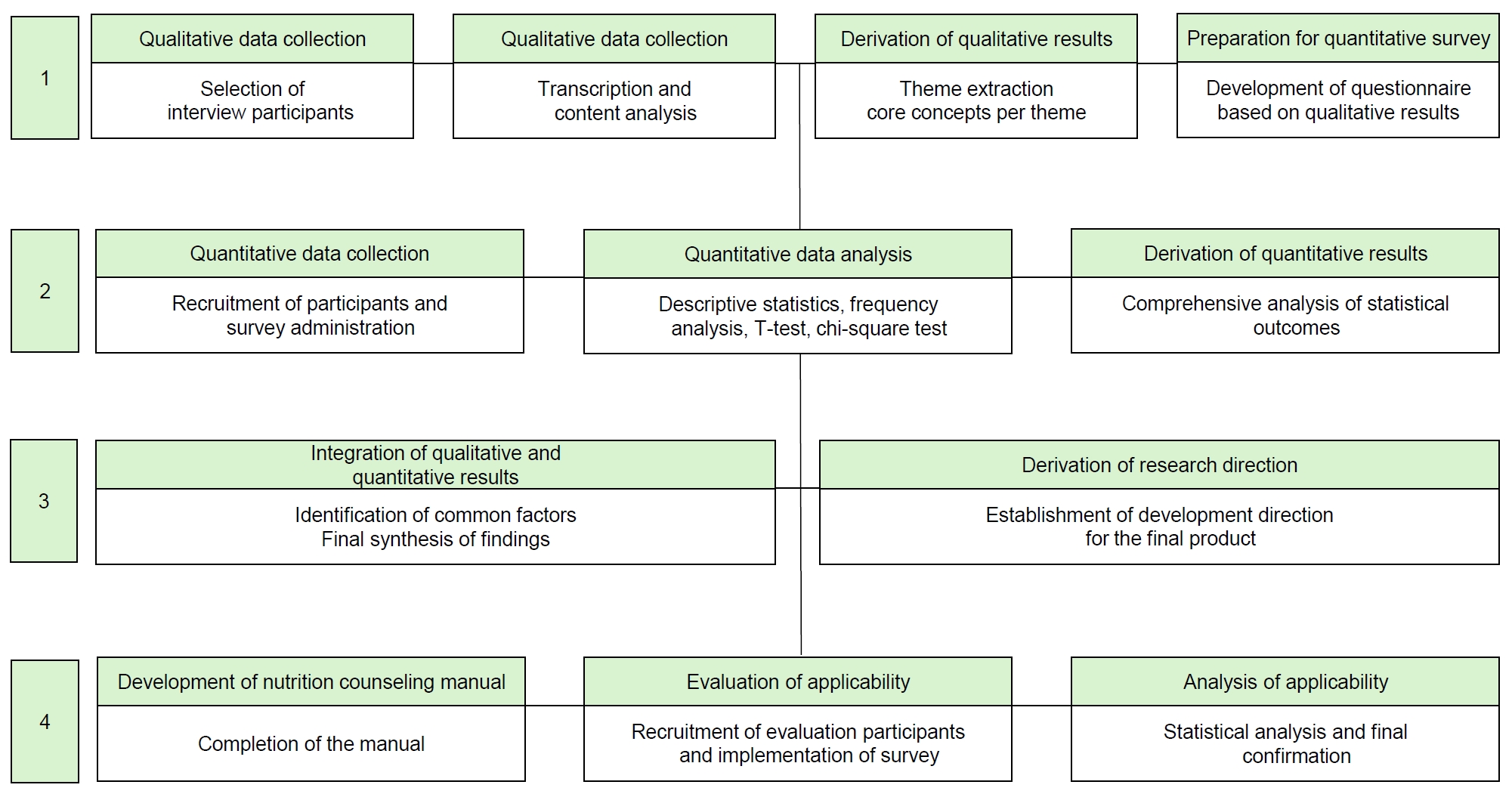
Fig. 2.Development of a nutrition counseling manual booklet and handbook for disability social welfare facilities. (A) Nutrition counseling manual guideline booklet. (B) Nutrition counseling manual handbook.
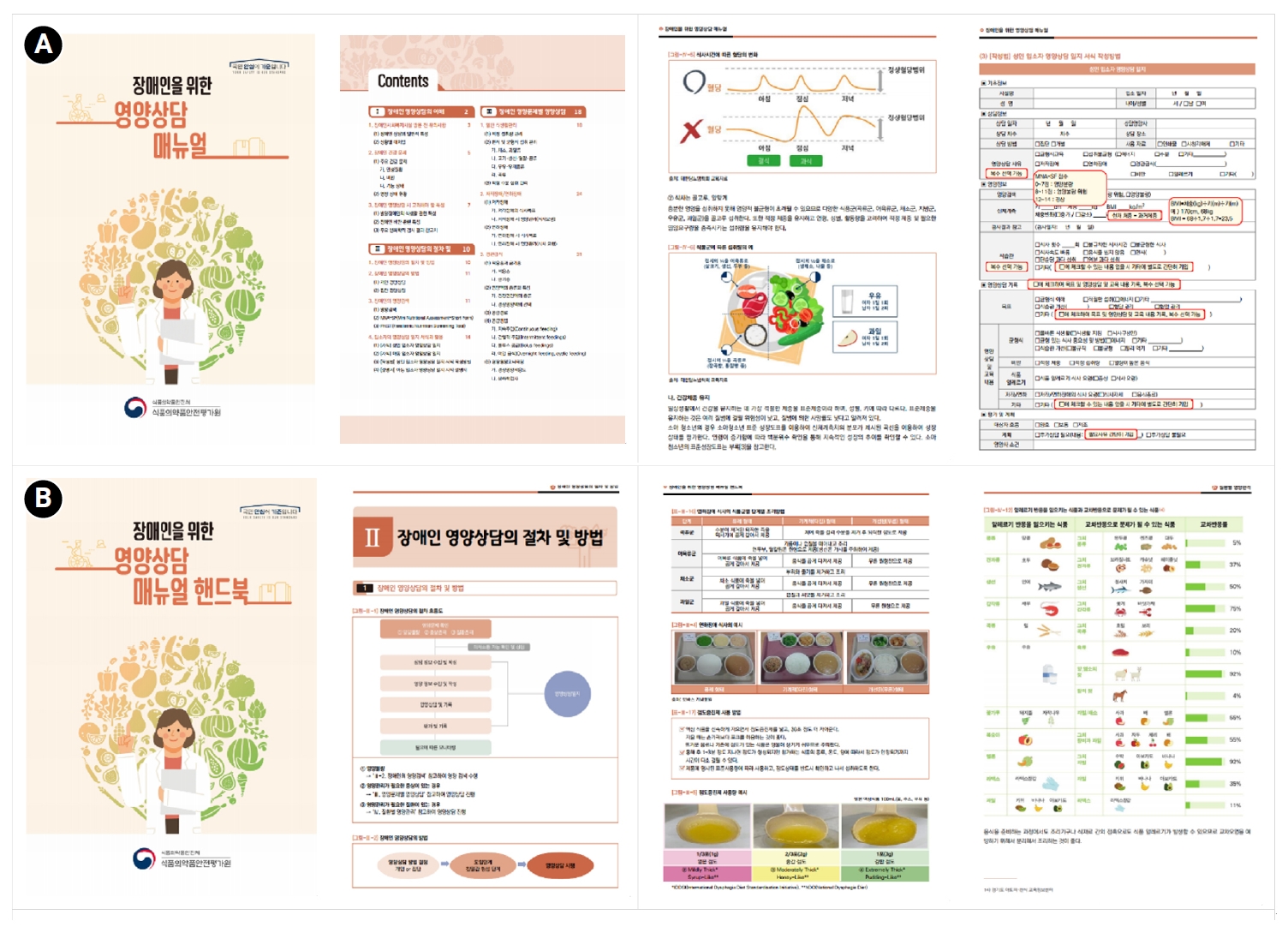
Table 1.General characteristics of in-depth interview participants: staff members of social welfare facilities
Table 2.Key findings on nutrition counseling materials for persons with disabilities
Table 3.General characteristics of survey respondents employed at facilities for persons with disabilities (n = 595)
| Categories | Variables | Value | |
|---|---|---|---|
| Respondents | Sex | Female | 181 (72.7) |
| Male | 68 (27.3) | ||
| Age (year) | 20–29 | 13 (5.2) | |
| 30–39 | 69 (27.7) | ||
| 40–49 | 110 (44.2) | ||
| 50–59 | 51 (20.5) | ||
| 60–69 | 6 (2.4) | ||
| Facility | Dietitian employment status | Yes | 61 (24.5) |
| No | 188 (75.5) | ||
| Operation type of meal service | On-site (self-operated/home-style) | 185 (74.3) | |
| On-site (contracted) | 18 (7.2) | ||
| Off-site (delivered meal) | 46 (18.5) | ||
| Residents/users1) | Type of disability | Developmental disabilities | 468 (78.7) |
| Physical disabilities | 44 (7.4) | ||
| Multiple disabilities (developmental + physical) | 83 (13.9) | ||
| Frequent disease | Obesity | 204 (34.3) | |
| Intellectual and developmental disabilities | 103 (17.3) | ||
| Hypertension | 100 (16.8) | ||
| Diabetes | 95 (16.0) | ||
| Swallowing disorders | 35 (5.9) | ||
| Underweight | 22 (3.7) | ||
| Dyslipidemia | 15 (2.5) | ||
| Cardiovascular diseases | 5 (0.8) | ||
| Others | 16 (2.7) | ||
| Total | 595 (100) | ||
Table 4.Status of nutrition counseling services in facilities for persons with disabilities (n = 249)
Table 5.Perceptions of staff on nutrition counseling and educational topic needs for persons with disabilities in social welfare facilities (n = 249)
Table 6.General characteristics of respondents employed at 24 Center for Social Welfare Foodservice Management (n = 26)
Table 7.Results of the evaluation on the usefulness of nutrition counseling materials provided by the Center for Social Welfare Foodservice Management (n = 26)
| Categories | Variables | Value |
|---|---|---|
| Nutrition counseling manual | Inclusion of necessary topics | 4.30 ± 0.691) |
| Appropriateness of content | 4.13 ± 0.61 | |
| Intention to use | 4.13 ± 0.80 | |
| Level of utilization | 3.96 ± 0.86 | |
| Satisfaction level | 3.87 ± 0.74 | |
| Effectiveness in improving nutritional status | 3.74 ± 0.99 | |
| Convenience of checking the information | 3.70 ± 0.95 | |
| (Average) | 3.98 ± 0.80 |
Table 8.Composition of the nutrition counseling manual and handbook for facilities for persons with disabilities
- 1. Lee HS. Foodservice management and food sanitation management in the welfare institutions for the disabled in Korea. Korean J Community Nutr 2008; 13(4): 520-530.
- 2. Byun YC, Kim SH, Yoon SY, Bae HO, Park SM, Choi MY. A study on systematic income security for the disabled in Korea. Korea Institute for Health and Social Affairs; 2004 Dec. Report No. 2004-15.
- 3. Choi H. A study on services direction of people with developmental disabilities who live in residential institution. [master’s thesis]. Konkuk University; 2020.
- 4. Seo W, Seo WY, Lee S. A qualitative study on suicidal ideation and suicidal attempts of people with disabilities and their family members. Disabil Soc Welf 2019; 10(2): 85-114.
- 5. Kwon JS, Lee HS. Nutrient intakes and the physical activities of the mentally retarded persons according to the degree of handicap who were accommodated in institutions in Andong area. Korean J Community Nutr 2007; 12(6): 790-797.
- 6. Kim JY. Effects of exercise and nutrition education program on physical fitness and dietary habits for intellectual disabilities. Korea J Sport 2018; 16(3): 355-362.
- 7. Kim SY. Investigating the mediation path of eating habits on the relationship between the subjective reporting of obesity and life satisfaction. J Humanit Soc Sci 2022; 30(4): 96-118.
- 8. American Dietetic Association. Providing nutrition services for infants, children, and adults with developmental disabilities and special health care needs. J Am Diet Assoc 2004; 104(1): 97-107. ArticlePubMed
- 9. Kim JY, Kang MW, Seo WY, Lee JW. Chronic diseases, health behaviors, and mortality in persons with disabilities: an analysis of the National Health Insurance Service-Health Screening (NHIS-HEALS) database. Health Soc Welf Rev 2020; 40(2): 121-150.
- 10. Jung CS, Kim DW. Assessment of nutritional status and annual changes in biochemical indicators according to long-term food intake in individuals with intellectual disabilities living in welfare facilities. Culi Sci Hos Res 2018; 24(4): 52-62.
- 11. Lee HS. Factors influencing on the job satisfaction and the turnover intention of dietitians working in the institutions for the disabled in Korea : focused on the general characteristics and the job burnout. Korean J Community Nutr 2009; 14(2): 182-189.
- 12. Morad M, Nelson NP, Merrick J, Davidson PW, Carmeli E. Prevalence and risk factors of constipation in adults with intellectual disability in residential care centers in Israel. Res Dev Disabil 2007; 28(6): 580-586. ArticlePubMed
- 13. Bong YN, Kim SY. A systematic literature review on the effects of participation in exercise and nutrition intervention for people with bipolar disorder. Korean J Adapt Phys Act 2022; 30(3): 23-37.
- 14. Kim J, Han D, Oh J, Ryou HJ, Hwang JY, Kim K, et al. A study on the improvement of evaluation scheme for the installation and operation of Center for Children’s and Social Welfare Foodservice Management: utilizing interviews with center stakeholders and external experts. J Nutr Health 2024; 57(6): 685-698. ArticleLink
- 15. Lee BS. A study on perception of service provider about self-determination of people with intellectual disabilities. J Intellect Disabil 2016; 18(1): 77-97.
- 16. Na Y, Oh J, Lee KW. A qualitative study of changes in adolescent dietary behavior during the COVID-19 pandemic and improvement strategies for school-provided nutrition counseling. Hum Ecol Res 2023; 61(1): 39-51. Article
- 17. Yoo HY. The experience of relationships with persons with developmental disabilities perceived by social workers at residential facilities for the disabled. Korean J Qual Res Soc Welf 2016; 10(2): 5-39.
- 18. Choi M, Hwang I, Yoon T. Factors affecting the health inequality between people with and without disability: focusing on subjective health status. J Korean Data Anal Soc 2018; 20(2): 1021-1035.
- 19. Yang JS. Dietary behaviors, food preferences and physical activity of the mentally disabled residents in welfare institutes. [master’s thesis]. Wonkwang University; 2011.
- 20. Mercer KC, Ekvall SW. Comparing the diets of adults with mental retardation who live in intermediate care facilities and in group homes. J Am Diet Assoc 1992; 92(3): 356-358. ArticlePubMed
- 21. Korea Disabled People's Development Institute. A survey on the current status and operation of daycare facilities for people with disabilities. Korea Disabled People's Development Institute; 2019 Oct. Report No. 19-14.
- 22. Friedman C. Assistive technology for people with intellectual and developmental disabilities in the United States in Home- and Community-Based Services. Disabil Rehabil Assist Technol 2024; 19(6): 2213-2220. ArticlePubMed
- 23. Park SH, Kim BR. Nutrition education based on breathing alert effects of nutrient intake, weight and meal time in adults with developmental disabilities. Mindful Pract 2022; 5(1): 95-116; https://scholar.kyobobook.co.kr/article/detail/4010037054875.
- 24. Jang S. An analysis of the trends in qualitative studies in the area of welfare of people with disabilities. J Future Soc Work Res 2019; 10(2): 73-102.
- 25. Ministry of Health and Welfare (MOHW). 2022 Directory of disability welfare facilities. MOHW; 2022.
- 26. Choi Y, Lee J, Lim H, Park YK. Effectiveness of NQ-E index-based individual nutrition counseling for community-care elderly: an intervention study on improving nutritional status, complex chronic diseases, and quality of life. Korean J Community Nutrition 2023; 28(6): 480-494. ArticleLink
- 27. Choi BY, Kang KS. The effect of music therapy applying virtual reality for the intellectually disables’ eating behavior modification. J Korean Assoc Dev Disabil 2019; 23(1): 1-19. Article
- 28. Bae TJ, Jeon NE, Choi SK, Seo JS. Effect of nutrition counseling by nutrition care process on diet therapy practice and glycemic control in type 2 diabetic patients. Korean J Community Nutrition 2020; 25(3): 214-225. ArticleLink
- 29. Hwang JK. A qualitative case study on the community life of woman with intellectual disabilities. Korean Acad Qual Res Soc Welf 2021; 15(1): 5-40.
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
Cite- Figure
-
- We recommend
- Related articles
-
- A needs assessment for the development of a digital-based self-nutrition management education program for older adults in Korea: a cross-sectional study
- Development and applicability evaluation of a nutrition education program for residents and users of disability social welfare facilities in Korea: a mixed-methods study
A study on the development of nutrition counseling manual and curriculum for the disabled in Korea: a mixed-methods study
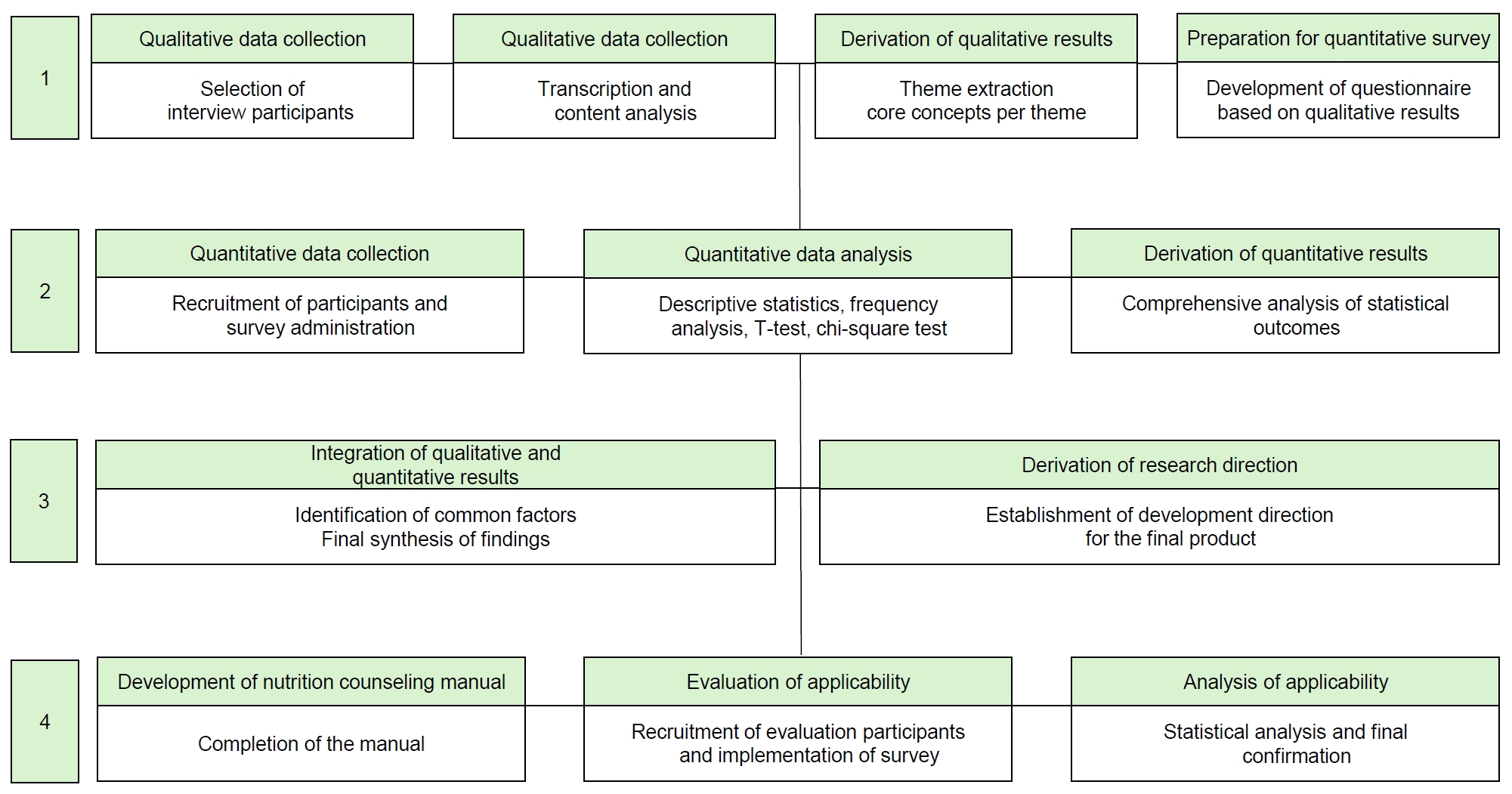
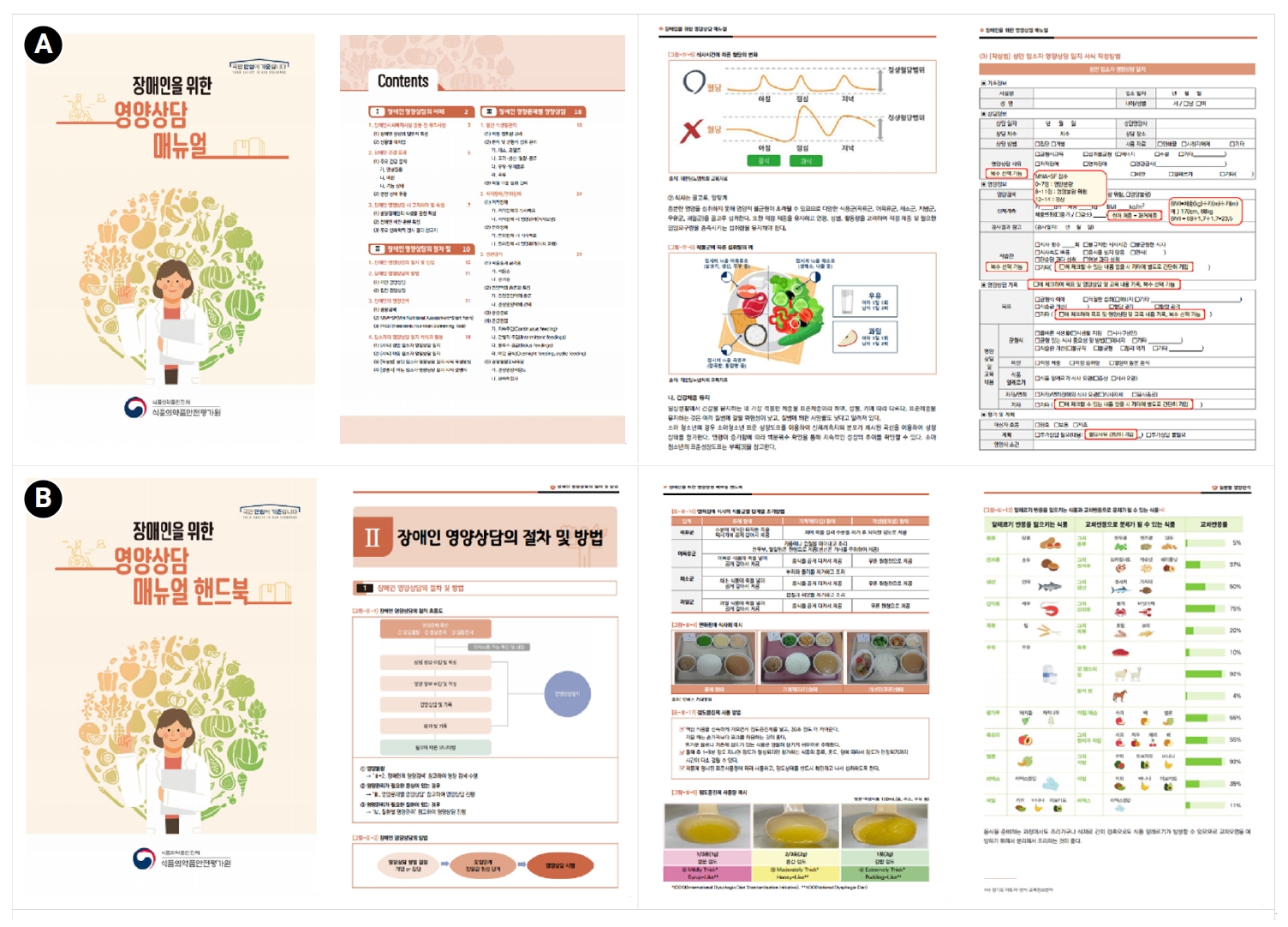
Fig. 1. Analytical stages of mixed methods research integrating qualitative and quantitative approaches.
Fig. 2. Development of a nutrition counseling manual booklet and handbook for disability social welfare facilities. (A) Nutrition counseling manual guideline booklet. (B) Nutrition counseling manual handbook.
Fig. 1.
Fig. 2.
A study on the development of nutrition counseling manual and curriculum for the disabled in Korea: a mixed-methods study
| Participant ID | Sex | Age group | Type of facility | Job title | Length of employment at facility | Length of employment in the health and welfare field |
|---|---|---|---|---|---|---|
| 1 | F | 50s | Residential facility for persons with disabilities | Cook | ≤ 1 year | ≤ 5 year |
| 2 | F | 60s | Residential facility for persons with disabilities | Manager (facility director) | ≥ 10 years | ≥ 20 years |
| 3 | F | 40s | Residential facility for persons with disabilities | Manager (facility director) | ≥ 10 years | ≥ 20 years |
| 4 | F | 40s | Residential facility for persons with disabilities | Nutritionist | 6–10 years | 5–10 years |
| 5 | M | 40s | Residential facility for persons with disabilities | Manager (department head) | ≥ 10 years | 16–20 years |
| 6 | F | 40s | Short-term residential facility for persons with disabilities | Manager (facility director) | ≥ 10 years | ≥ 20 years |
| 7 | F | 50s | Short-term residential facility for persons with disabilities | Cook | 3–5 years | 5–10 years |
| 8 | F | 30s | Day activity center for persons with disabilities | Manager (department head) | 3–5 years | ≤ 5 year |
| 9 | F | 40s | Short-term residential facility for persons with disabilities | Manager (facility director) | 1–2 years | ≥ 20 years |
| 10 | M | 50s | Short-term residential facility for persons with disabilities | Manager (facility director) | ≥ 10 years | ≥ 20 years |
| 11 | F | 40s | Short-term residential facility for persons with disabilities | Manager (deputy director) | ≥ 10 years | 11–15 years |
| Theme | Sub-theme | Constructed meaning |
|---|---|---|
| Education topics | - Various education topics | - Individuals with brain lesions cannot participate in education |
| - Nutrition education on various topics is needed for facility staff | ||
| - Educaion on stimulating eating interest and providing meal support | - Education is needed to guide healthy eating habits | |
| - Methods to stimulate interest in meals | ||
| - Professional training is required to support individuals with chewing or swallowing difficulties | ||
| - Basic nutrition education and fundamental cooking skills | - Basic nutrition education should be provided | |
| - Basic cooking training for male employees is recommended | ||
| - Food allergy management methods | - Guidance on providing alternative meals for food allergies is required | |
| - Training in food allergy management should be offered | ||
| Education media | - Customized materials for facility staff | - In-person training for facility staff is required |
| - Remote training with simple material distribution is ineffective | ||
| - Group sessions using PowerPoint materials are preferred | ||
| - Online and offline educational materials | - Materials should be usable independently within the facility | |
| - Materials should provide information for guardians | ||
| - Educational materials should be simple and accessible (e.g., card news, infographics, videos) |
| Categories | Variables | Value | |
|---|---|---|---|
| Respondents | Sex | Female | 181 (72.7) |
| Male | 68 (27.3) | ||
| Age (year) | 20–29 | 13 (5.2) | |
| 30–39 | 69 (27.7) | ||
| 40–49 | 110 (44.2) | ||
| 50–59 | 51 (20.5) | ||
| 60–69 | 6 (2.4) | ||
| Facility | Dietitian employment status | Yes | 61 (24.5) |
| No | 188 (75.5) | ||
| Operation type of meal service | On-site (self-operated/home-style) | 185 (74.3) | |
| On-site (contracted) | 18 (7.2) | ||
| Off-site (delivered meal) | 46 (18.5) | ||
| Residents/users |
Type of disability | Developmental disabilities | 468 (78.7) |
| Physical disabilities | 44 (7.4) | ||
| Multiple disabilities (developmental + physical) | 83 (13.9) | ||
| Frequent disease | Obesity | 204 (34.3) | |
| Intellectual and developmental disabilities | 103 (17.3) | ||
| Hypertension | 100 (16.8) | ||
| Diabetes | 95 (16.0) | ||
| Swallowing disorders | 35 (5.9) | ||
| Underweight | 22 (3.7) | ||
| Dyslipidemia | 15 (2.5) | ||
| Cardiovascular diseases | 5 (0.8) | ||
| Others | 16 (2.7) | ||
| Total | 595 (100) | ||
| Category | Item | Frequency |
|---|---|---|
| Provision of nutrition counseling | Yes | 71 (28.5) |
| No | 178 (71.5) | |
| Total | 249 (100) | |
| Frequency of nutrition counseling | Twice a month | 1 (1.4) |
| Once a month | 15 (21.1) | |
| Once every 2–3 months | 6 (8.5) | |
| Once or twice a year | 8 (11.3) | |
| Once a year | 10 (14.1) | |
| On an irregular basis | 27 (38.0) | |
| Others | 4 (5.6) | |
| Total | 71 (100) | |
| Provider of nutrition counseling | In-house facility staff | 62 (87.3) |
| External agencies (e.g., local government, organizations) | 3 (4.2) | |
| Hospitals | 3 (4.2) | |
| Public health centers | 3 (4.2) | |
| Total | 71 (100) | |
| Reasons for not providing nutrition counseling | Lack of educational materials and guidelines | 49 (27.5) |
| Difficulties in direct counseling with residents/users | 44 (24.7) | |
| Limited knowledge about counseling | 38 (21.3) | |
| Heavy administrative workload of staff | 29 (16.3) | |
| Lack of awareness of the need for counseling | 7 (3.9) | |
| Low perceived effectiveness of counseling | 2 (1.1) | |
| Others | 9 (5.1) | |
| Total | 178 (100) |
| Categories | Variables | Value |
|---|---|---|
| Perceptions of staff on nutrition counseling | Improvement in the health of residents/users | 4.04 ± 0.89 |
| Enhancement of residents’/users’ life satisfaction | 4.01 ± 0.93 | |
| Dependence on nutrition counseling services | 4.00 ± 0.91 | |
| Necessity of nutrition counseling for caregivers | 3.86 ± 1.02 | |
| (Average) | 3.98 ± 0.94 | |
| Educational topic needs | Personal hygiene | 4.44 ± 0.71 |
| Accident prevention | 4.41 ± 0.72 | |
| Obesity management | 4.34 ± 0.74 | |
| Food poisoning prevention | 4.23 ± 0.82 | |
| Convenience food management | 4.18 ± 0.90 | |
| Sugar intake management | 4.02 ± 0.89 | |
| Safe food choices | 4.00 ± 0.87 | |
| Healthy snacking | 3.92 ± 0.87 | |
| Processed food awareness | 3.87 ± 0.85 | |
| Low-sodium diet | 3.86 ± 0.90 | |
| Dietary supplement | 3.69 ± 0.98 | |
| Hydration | 3.68 ± 1.00 | |
| Digestive disorders | 3.43 ± 1.00 | |
| Bowel disorders | 3.40 ± 1.06 | |
| Management of preference foods | 3.24 ± 1.26 | |
| Dysphagia | 3.22 ± 1.22 | |
| Underweight | 2.98 ± 1.20 | |
| (Average) | 3.82 ± 0.88 |
| Categories | Variables | Value |
|---|---|---|
| Working period | Less than 1 year | 3 (11.5) |
| 1 year or more to less than 5 years | 13 (50.0) | |
| 5 years or more | 10 (38.5) | |
| Type of license | Clinical dietitian | 9 (34.6) |
| Dietitian | 17 (65.4) |
| Categories | Variables | Value |
|---|---|---|
| Nutrition counseling manual | Inclusion of necessary topics | 4.30 ± 0.69 |
| Appropriateness of content | 4.13 ± 0.61 | |
| Intention to use | 4.13 ± 0.80 | |
| Level of utilization | 3.96 ± 0.86 | |
| Satisfaction level | 3.87 ± 0.74 | |
| Effectiveness in improving nutritional status | 3.74 ± 0.99 | |
| Convenience of checking the information | 3.70 ± 0.95 | |
| (Average) | 3.98 ± 0.80 |
| Categories | Variables | Detailed content |
|---|---|---|
| Ⅰ. General understanding of nutrition counseling | Pre-counseling guide for understanding nutritional needs of persons with disabilities | - Communication strategies by disability type (cognitive impairment, speech difficulty) |
| - Nutrition intervention rationale (undernutrition, obesity, metabolic risk) | ||
| - Eating behavior traits (food selectivity, sensory issues, disordered eating) | ||
| Ⅱ. Procedures and methods | Field-ready counseling guidelines with simplified tools | - Disability-specific tools (MNA-SF, PNST) |
| - Practical templates for documentation | ||
| Ⅲ–Ⅳ. Counseling for Specific Issues | Summary of nutrition strategies and interventions for key conditions | - Counseling by nutrition issues (chewing, enteral feeding, diet balance) |
| - Counseling by disease (diabetes, obesity, food allergy) | ||
| Ⅴ-Ⅶ. Reference materials | Organized resources for efficient counseling | - Growth charts, height estimation, essential forms |
| - Useful websites and educational handouts | ||
| Ⅷ. References | Supporting scientific validity and reliability | - Reference list used in manual development |
Table 1. General characteristics of in-depth interview participants: staff members of social welfare facilities
M, male; F, female.
Table 2. Key findings on nutrition counseling materials for persons with disabilities
Table 3. General characteristics of survey respondents employed at facilities for persons with disabilities (n = 595)
n (%). Multiple responses.
Table 4. Status of nutrition counseling services in facilities for persons with disabilities (n = 249)
n (%).
Table 5. Perceptions of staff on nutrition counseling and educational topic needs for persons with disabilities in social welfare facilities (n = 249)
Mean ± SD. 5-point Likert scale (1: not at all, 5: very much).
Table 6. General characteristics of respondents employed at 24 Center for Social Welfare Foodservice Management (n = 26)
n (%).
Table 7. Results of the evaluation on the usefulness of nutrition counseling materials provided by the Center for Social Welfare Foodservice Management (n = 26)
Mean ± SD. 5-point Likert scale (1: not at all, 5: very much). Out of 5.0.
Table 8. Composition of the nutrition counseling manual and handbook for facilities for persons with disabilities
MNA-SF, Mini Nutritional Assessment Short Form; PNST, Paediatric Nutrition Screening Tool.


