
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 23(1); 2018 > Article
-
Research Article
- Effect of Active Nutrition Care on Underweight Elderly Patients Receiving Long-term Enteral Tube Feeding
-
Hwa-Young Yoon, Hye-Kyeong Kim

-
Korean Journal of Community Nutrition 2018;23(1):48-59.
DOI: https://doi.org/10.5720/kjcn.2018.23.1.48
Published online: February 28, 2018
Department of Food Science & Nutrition, The Catholic University of Korea, Bucheon, Korea.
- Corresponding author: Hye-Kyeong Kim. Department of Food Science & Nutrition, The Catholic University of Korea, 43 Jibongro, Wonmi-gu, Bucheon, Gyeonggi-do 14662, Korea. Tel: (02) 2164-4314, Fax: (02) 2164-4314, hkyeong@catholic.ac.kr
• Received: February 7, 2018 • Revised: February 21, 2018 • Accepted: February 21, 2018
Copyright © 2018 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,844 Views
- 8 Download
- 1 Crossref

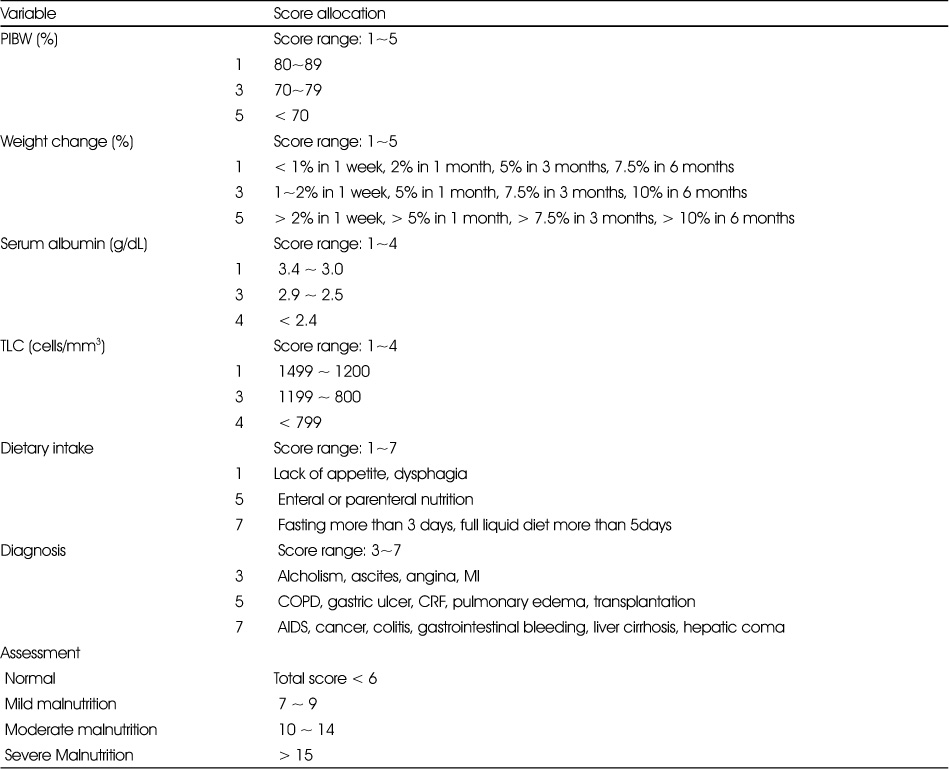
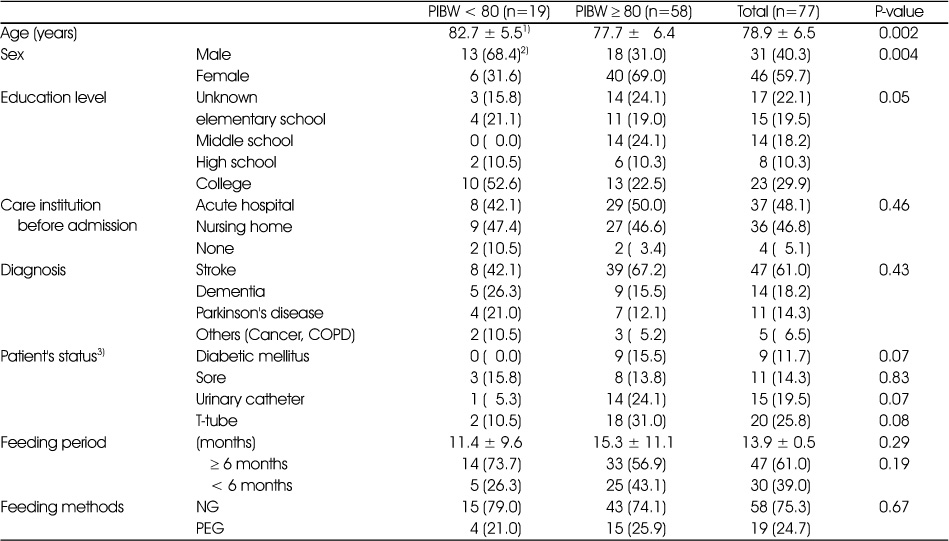




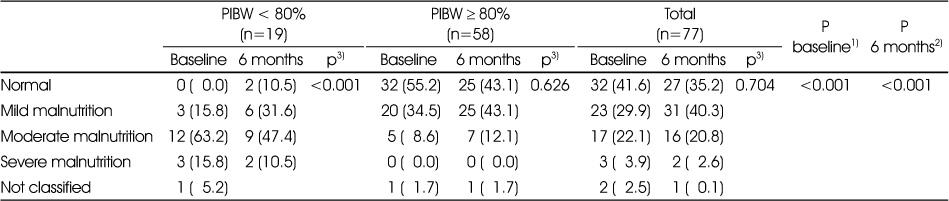
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- The Status of Enteral Nutrition Formula Use by Dietitians in Hospitals Within Busan and Gyeongnam Area
Haejin Kang, Minji Woo, Eunju Park, Yoo Kyoung Park
Clinical Nutrition Research.2022; 11(1): 9. CrossRef
 Cite
CiteEffect of Active Nutrition Care on Underweight Elderly Patients Receiving Long-term Enteral Tube Feeding

Fig. 1
The protocol of the study
Fig. 1
Effect of Active Nutrition Care on Underweight Elderly Patients Receiving Long-term Enteral Tube Feeding
Nutritional risk screening
PIBW; percentage of ideal body weight, MI; myocardiac infarction, COPD; chronic obstructive pulmonary disease, CRF; chronic renal failure, AIDS; acquired immune deficiency syndrome
General characteristics of the patients
PIBW; percent of ideal body weight, COPD; chronic obstructive pulmonary disease, T-tube; tracheostomy tube, NG: nasogastric tube, PEG: percutaneous endoscopic gastrostomy tube
1) Means ± SD, 2) N (%), 3) Patient's status to each item were checked and the result is the rate of ‘yes’ to each item
Change of enteral feeding status during 6 months of nutrition support
RC; required calorie, SC; supplied calorie, SRC; supply to required calorie, RP; required protein, SP; supplied protein, SRP; supply to required protein, PIBW; percent ideal body weight
1) Means ± SD, Mean values with different superscripts are significantly different among the time points in each group at p<0.05 as determined by ANOVA and Duncan's multiple range test, 2) N (%), *: p<0.05, **: p<0.01, ***: p<0.0001 between groups
Incidence of feeding intolerance during 6 months of nutrition support
PIBW; percent ideal body weight
1) Percent (%) of patients with each intolerance. Feeding intolerance was checked daily for the first 3 months after admission and when referral from doctor was given thereafter.
Change of anthropometric data during 6 months of nutrition support
PIBW; percent of ideal body weight, BMI; body mass index
1) Means ± SD, Mean values with different superscripts are significantly different among the time points in each group at p<0.05 as determined by ANOVA and Duncan's multiple range test
*: p<0.05 between groups
Change of laboratory data during 6 months of nutrition support
GOT : glutamate oxalacetate transaminase, GPT: glutamate pyruvate transaminase, TP: total protein, ALB: albumin, TC: total cholesterol, HDL-c: high density lipoprotein cholesterol, TG: triglyceride, LDL-c: low density lipoprotein cholesterol, Hb: hemoglobin, Hct: hematocrit, TLC: total lymphocyte count, PIBW; percent ideal body weight, N/A; not available
1) Means ± SD, Mean values with different superscripts are significantly different among the time points in each group at p<0.05 as determined by ANOVA and Duncan's multiple range test
*: p<0.05 between groups
Change of nutritional status during 6 months of nutrition support
1) P value from chi-square test between groups at baseline
2) P value from chi-square test between groups after 6 months of nutrition support
3) P value from chi-square test between baseline and 6 months in each group
Table 1
Nutritional risk screening
PIBW; percentage of ideal body weight, MI; myocardiac infarction, COPD; chronic obstructive pulmonary disease, CRF; chronic renal failure, AIDS; acquired immune deficiency syndrome
Table 2
General characteristics of the patients
PIBW; percent of ideal body weight, COPD; chronic obstructive pulmonary disease, T-tube; tracheostomy tube, NG: nasogastric tube, PEG: percutaneous endoscopic gastrostomy tube 1) Means ± SD, 2) N (%), 3) Patient's status to each item were checked and the result is the rate of ‘yes’ to each item
Table 3
Change of enteral feeding status during 6 months of nutrition support
RC; required calorie, SC; supplied calorie, SRC; supply to required calorie, RP; required protein, SP; supplied protein, SRP; supply to required protein, PIBW; percent ideal body weight 1) Means ± SD, Mean values with different superscripts are significantly different among the time points in each group at p<0.05 as determined by ANOVA and Duncan's multiple range test, 2) N (%), *: p<0.05, **: p<0.01, ***: p<0.0001 between groups
Table 4
Incidence of feeding intolerance during 6 months of nutrition support
PIBW; percent ideal body weight 1) Percent (%) of patients with each intolerance. Feeding intolerance was checked daily for the first 3 months after admission and when referral from doctor was given thereafter.
Table 5
Change of anthropometric data during 6 months of nutrition support
PIBW; percent of ideal body weight, BMI; body mass index 1) Means ± SD, Mean values with different superscripts are significantly different among the time points in each group at p<0.05 as determined by ANOVA and Duncan's multiple range test *: p<0.05 between groups
Table 6
Change of laboratory data during 6 months of nutrition support
GOT : glutamate oxalacetate transaminase, GPT: glutamate pyruvate transaminase, TP: total protein, ALB: albumin, TC: total cholesterol, HDL-c: high density lipoprotein cholesterol, TG: triglyceride, LDL-c: low density lipoprotein cholesterol, Hb: hemoglobin, Hct: hematocrit, TLC: total lymphocyte count, PIBW; percent ideal body weight, N/A; not available 1) Means ± SD, Mean values with different superscripts are significantly different among the time points in each group at p<0.05 as determined by ANOVA and Duncan's multiple range test *: p<0.05 between groups
Table 7
Change of nutritional status during 6 months of nutrition support
1) P value from chi-square test between groups at baseline 2) P value from chi-square test between groups after 6 months of nutrition support 3) P value from chi-square test between baseline and 6 months in each group


