
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 31(1); 2026 > Article
-
Review
국내 발달장애인 식생활 및 영양교육 연구동향: 주제범위 문헌고찰(2015–2025) -
곽나경1),*
 , 박원영2),*, 김유리3), 오지은4),†
, 박원영2),*, 김유리3), 오지은4),† - Research trends in dietary behaviors and nutrition education among individuals with developmental disabilities in Korea: a scoping review (2015–2025)
-
Nakyung Kwak1),*, Wonyeong Park2),*, Yu-Ri Kim3), Jieun Oh4),†
-
Korean Journal of Community Nutrition 2026;31(1):1-20.
DOI: https://doi.org/10.5720/kjcn.2025.00374
Published online: February 28, 2026
1)이화여자대학교 임상보건학과 석사과정생
2)이화여자대학교 식품영양학과 석사과정생
3)이화여자대학교 특수교육학과 교수
4)이화여자대학교 신산업융합대학 교수
1)M.S. Student, Department of Clinical Healthcare, Ewha Womans University, Seoul, Korea
2)M.S. Student, Department of Nutritional Science and Food Management, Ewha Womans University, Seoul, Korea
3)Professor, Department of Special Education, Ewha Womans University, Seoul, Korea
4)Professor, College of Science and Industry Convergence, Ewha Womans University, Seoul, Korea
- †Corresponding author: Jieun Oh College of Science and Industry Convergence, Ewha Womans University, 52 Ewhayeodae-gil, Seodaemun-gu, Seoul 03760, Korea Tel. +82-2-3277-6586 Fax: +82-2-3277-6586 Email: oje96@ewha.ac.kr
• Received: December 31, 2025 • Revised: February 1, 2026 • Accepted: February 23, 2026
© 2026 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,295 Views
- 69 Download
Abstract
-
Objectives
- We mapped trends in studies on dietary behaviors, nutritional status, and nutrition-related education among individuals with developmental disabilities in Korea over the past decade to identify research gaps and inform future research and policy development.
-
Methods
- A scoping review was conducted using three major Korean academic databases (RISS, KISS, and DBpia). Studies published between 2015 and September 2025 were identified using combinations of keywords related to developmental disabilities, dietary behavior, nutrition, and health-related interventions. Eligible studies included empirical studies and secondary research (e.g., systematic or scoping reviews) conducted in Korea that focused on dietary behaviors, nutrition, health promotion, or nutrition-related education for individuals with developmental disabilities. Thirty-six studies met our inclusion criteria and were analyzed based on study design, study population, disability type, research topic, and publication period.
-
Results
- Observational quantitative, qualitative, intervention-based experimental, and evidence synthesis accounted for 27.8%, 13.9%, 22.2%, and 36.1% of all included studies, respectively. Children and adolescents (27.8%) and adults (25.0%) were the most frequently studied populations, with limited studies focusing on professionals or teachers. Most studies targeted individuals with developmental disabilities as a combined group (61.1%), followed by those specifically targeting autism spectrum disorder. Research topics included dietary behaviors and nutritional status, nutrition-related education and interventions, health promotion, and medical or clinical issues, with many small-scale and short-term intervention studies.
-
Conclusion
- Although research on dietary and nutrition-related issues among individuals with developmental disabilities in Korea has expanded in scope and methodology, significant limitations remain. Future research should adopt longitudinal and community-based approaches, incorporate diverse populations, and strengthen policy-oriented nutrition support systems to promote sustainable health and quality of life for individuals with developmental disabilities.
INTRODUCTION
METHODS
RESULTS
DISCUSSION
-
CONFLICT OF INTEREST
The authors declare no financial or other issues that might lead to conflict of interest.
-
FUNDING
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2025S1A5A2A03016997).
-
DATA AVAILABILITY
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
NOTES
Fig. 1.Flow diagram of the literature selection process (adapted from the Joanna Briggs Institute scoping review methodology).
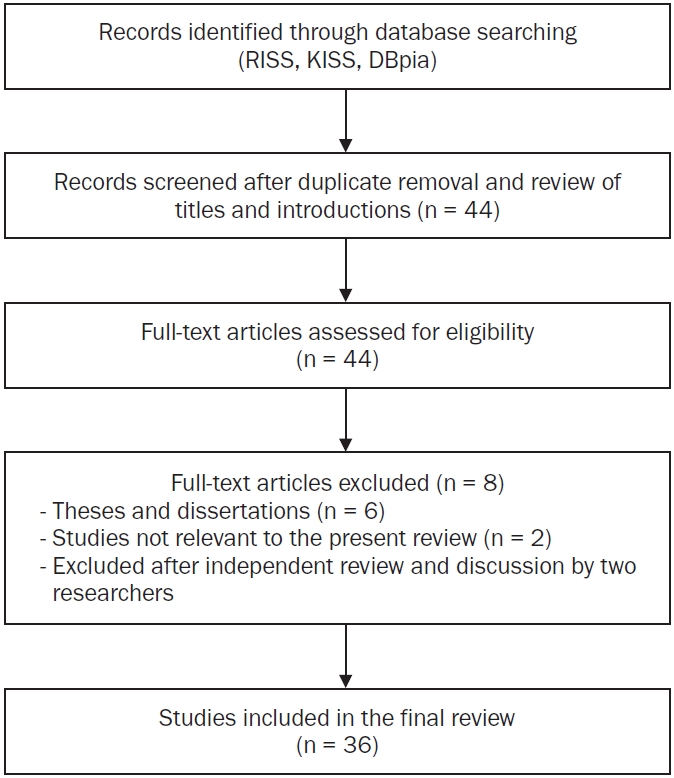
Table 1.Literature search strategy and keyword combinations
Table 2.Characteristics of included studies
| Study ID | Reference | Population | Disability type | Study design | Main topic | Key findings |
|---|---|---|---|---|---|---|
| S1 | Kim et al. [19] (2025) | Adults with developmental disabilities | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Physical activity and health promotion | Included studies primarily targeted adults with mild to moderate intellectual disabilities and most frequently used single-group pre–post designs. Interventions reported overall positive changes in anthropometric measures, physical fitness, physical activity levels, dietary behaviors, health knowledge, self-efficacy, and quality of life. Few studies assessed maintenance/generalization, intervention fidelity, or social validity. Programs mainly focused on nutrition education, physical activity information, and exercise participation, frequently using visual supports and reinforcement strategies |
| S2 | Kim [21] (2024) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Dietary habits and nutritional status | Domestic studies have increased since 2012, with most employing literature reviews or survey designs. Qualitative and intervention studies were relatively scarce, and study populations were concentrated on children and individuals with multiple disabilities. Common dietary behavior issues included food selectivity, texture sensitivity, fear of new foods, pica, and atypical eating patterns |
| S3 | Ahn et al. [22] (2015) | Adults with developmental disabilities | Mixed disability groups | Observational quantitative studies (cross-sectional survey) | Dietary habits and nutritional status | Mean BMI indicated overweight in the intellectual disability group and obesity in the mental disability group. Intake frequencies of vegetables and dairy products were generally low. Both groups showed vitamin B1, B2, and calcium intakes below recommended levels. Carotenoid intake, particularly lycopene, was lower than that of the general population, and cryptoxanthin intake was also low in the mental disability group |
| S4 | Lee et al. [23] (2018) | Mixed (overlapping) | Developmental disabilities (overall) | Exploratory qualitative studies (in-depth interviews and focus groups; constant comparative analysis) | Medical, health and clinical topics | Key findings included difficulties in expressing and recognizing illness and symptoms, practical challenges in health management, barriers in access and communication during medical encounters, and limited self-determination in healthcare. Individuals with developmental disabilities experienced restricted access to information and decision-making due to communication difficulties and reliance on caregivers, with lack of disability awareness, inadequate facilities, and financial burden identified as major barriers |
| S5 | Kim et al. [24] (2021) | Professionals and teachers | Autism spectrum disorder | Exploratory qualitative studies (in-depth interviews and focus groups; constant comparative analysis) | Dietary habits and nutritional status | Major themes included types of eating behaviors, eating-related problems, influencing factors (individual, environmental, medical), coping and instructional strategies, instructional difficulties, and support needs. Common eating behavior problems among students with ASD included food selectivity, texture sensitivity, food refusal, and pica, with gastrointestinal symptoms, sensory and behavioral characteristics, and home–school environments interacting to influence eating behaviors |
| S6 | Lee et al. [25] (2022) | Children and adolescents with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (single-group pre–post) | Nutrition and dietary education or interventions | Following the health education intervention, students’ health knowledge and health-promoting behavior scores significantly increased compared with baseline. Ninety-three percent of participants achieved health management goals at or above the expected level. Self-determination significantly increased in student self-ratings, whereas no significant changes were observed in parent or teacher ratings |
| S7 | Kang & Lee [26] (2015) | Adults with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (randomized controlled pre–post design) | Physical activity and health promotion | Muscle mass increased most in the APA + Wii group, whereas body fat mass decreased most in the APA group. Muscular endurance, strength, flexibility, and cardiorespiratory fitness improved more in groups including APA than in the Wii-only group, while balance improved most in the Wii group. Step counts and caloric expenditure increased in all intervention groups compared with controls |
| S8 | Lee & Kim [27] (2024) | Parents and caregivers | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Medical, health and clinical topics | Depression intervention programs for families of individuals with developmental disabilities showed overall significant reductions in depressive symptoms. Most programs were short-term (fewer than 10 sessions) group-based interventions, with reported effect sizes in the moderate to large range |
| S9 | Shin et al. [28] (2024) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (scoping review) | Medical, health and clinical topics | Regular health checkups were identified as the most highly needed healthcare service. Across the life course, early diagnosis and early intervention were prioritized in infancy, whereas prevention of early aging and medical support were emphasized in middle and older adulthood. Individuals with developmental disabilities exhibited higher prevalence of chronic diseases, increased risk of premature mortality, and lower access to healthcare services, indicating substantial health vulnerability |
| S10 | Kim & Song [29] (2018) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (meta-analysis) | Nutrition and dietary education or interventions | The overall intervention effect size was Tau-U = 0.876, indicating moderate to high effectiveness. Larger effects were observed at younger ages and during follow-up phases compared with intervention phases. Multicomponent interventions were more effective than single-technique approaches, with the greatest effects reported for interventions lasting less than 20 sessions and approximately 2 months (5–8 weeks) |
| S11 | Min & Kim [30] (2024) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (narrative review) | Dietary habits and nutritional status | Feeding disorders in children with ASD were reported to be highly diverse, highlighting the need for comprehensive assessment. Available assessment tools were limited, and the inclusion of additional domains such as oral-motor and digestive function was recommended |
| S12 | Park et al. [31] (2020) | Mixed (overlapping) | Autism spectrum disorder | Observational quantitative studies (cross-sectional survey) | Dietary habits and nutritional status | BMI distribution differed by age, with higher rates of underweight among children aged ≤ 10 years and higher rates of overweight and obesity among adolescents aged 11–19 years. Most participants consumed snacks at least once daily. Food preferences differed across age groups for grains, vegetables, fruits, dairy products, fats, and sugars. Parents reported high needs and willingness to participate in nutrition education |
| S13 | Lee et al. [32] (2016) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Observational quantitative studies (retrospective medical record review) | Medical, health and clinical topics | At the first visit, children with ASD had a higher proportion of males, fewer obstetric complications, and lower receptive and expressive language scores than children with intellectual disabilities. Children whose diagnosis changed from intellectual disability to ASD were all male, had more frequent family histories of developmental delay, and showed significantly lower initial receptive language scores. Sex, language characteristics, and obstetric information were associated with early ASD identification |
| S14 | Jeon & Cho [33] (2018) | Children and adolescents with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (single-case design) | Medical, health and clinical topics | After intervention, meal intake increased to approximately 700–800 g, with reductions in frequent small meals and shorter mealtime duration. Feeding patterns shifted from predominantly formula-based intake (≥ 80%) to mixed feeding after one week and to 100% solid food intake after two weeks. Applied behavior analysis intervention was associated with reductions in food refusal behaviors |
| S15 | Kim [34] (2022) | Adults with developmental disabilities | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional survey with mediated regression analysis) | Dietary habits and nutritional status | Higher levels of perceived obesity were associated with poorer dietary habits and lower life satisfaction. Regular meals and balanced nutrition were positively correlated with both dietary habit scores and life satisfaction. Dietary habits showed a significant mediating effect in the relationship between perceived obesity and life satisfaction |
| S16 | Oh & Hong [35] (2025) | Adults with developmental disabilities | Developmental disabilities (overall) | Evidence synthesis studies (narrative review) | Medical, health and clinical topics | Individuals with developmental disabilities showed reduced gut microbiota diversity, increased harmful bacteria, and decreased beneficial bacteria, which were associated with neurotransmitter dysregulation, immune and inflammatory responses, and metabolic imbalance. Dietary modification, probiotic supplementation, and physical activity interventions were reported to improve gut microbiota balance and related metabolic pathways |
| S17 | Kim [36] (2018) | Adults with developmental disabilities | Intellectual disability | Evidence synthesis studies (single-group pre–post) | Physical activity and health promotion | After 16 weeks of intervention, no significant changes were observed in body composition indicators (BMI, body fat percentage). However, flexibility, muscular strength, and power significantly improved. Dietary habit scores increased, with higher intake frequencies of protein, green-yellow vegetables, and seaweed, and reduced intake of salty foods, sweets, and late-night snacks |
| S18 | Choi & Kang [37] (2019) | Adults with developmental disabilities | Intellectual disability | Intervention-based experimental studies (multiple-baseline single-subject design) | Physical activity and health promotion | All participants showed increased numbers of appropriate eating behaviors during intervention and maintenance phases compared with baseline. Mean performance increased from 3.2 of 13 behaviors at baseline to 7 during intervention and 11 during maintenance. VR-based social story music therapy was associated with improvements in eating behavior performance and social skill acquisition |
| S19 | Kang & Kim [38] (2020) | Parents and caregivers | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional survey with hierarchical multiple regression) | Dietary habits and nutritional status | Poorer health status and higher levels of challenging behaviors in adults with developmental disabilities were significantly associated with increased caregiver burden. Health status and challenging behaviors were identified as significant predictors of caregiver burden |
| S20 | Kim et al. [39] (2020) | Parents and caregivers | Autism spectrum disorder | Exploratory qualitative studies (thematic analysis of in-depth interviews) | Dietary habits and nutritional status | Mothers’ experiences were categorized into themes related to children’s eating characteristics (clear food preferences, atypical eating behaviors, influence of past experiences), family interactions, efforts to improve dietary behaviors, and support needs. Children’s eating behavior problems imposed burdens on family meals, dining out, and mealtime atmosphere, with coping strategies involving environmental modification, consistent guidance, and program participation |
| S21 | Kim [40] (2016) | Parents and caregivers | Developmental disabilities (overall) | Intervention-based experimental studies (non-equivalent control group pre–post–follow-up design) | Nutrition and dietary education or interventions | Compared with the control group, the intervention group showed significantly greater improvements in children’s health management behaviors over time. Parenting stress scores in the intervention group significantly decreased at post-test and follow-up, with larger reductions than those observed in the control group |
| S22 | Kim & Jeon [41] (2024) | Professionals and teachers | Developmental disabilities (overall) | Exploratory qualitative studies (one-on-one in-depth interviews) | Nutrition and dietary education or interventions | The most frequently requested nutrition education topics were diet education for obesity prevention and management and basic nutrition knowledge. Education at kindergarten to lower elementary school level was considered appropriate given cognitive functioning. Activity-based, face-to-face education using real foods, cooking activities, and visual materials, delivered in sessions of approximately 30 minutes, was perceived as effective |
| S23 | Ham & Sohn [42] (2023) | Mixed (overlapping) | Developmental disabilities (overall) | Observational quantitative studies (secondary data analysis with two-way ANOVA) | Dietary habits and nutritional status | Smoking, alcohol consumption, and stress showed significant main effects across both life stage and sex. Overweight showed a significant main effect by life stage, whereas sexual health issues differed by sex. Significant interaction effects between life stage and sex were observed for all five health behaviors, with higher levels reported for specific subgroups such as adolescent males’ sexual health issues and older adults’ alcohol use or overweight |
| S24 | Park et al. [43] (2019) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (narrative review) | Dietary habits and nutritional status | Many studies reported that children with ASD exhibited atypical eating behaviors such as food selectivity, binge eating, and pica compared with typically developing children. Data collection relied mainly on parent reports and observations. Associations between eating behaviors and individual characteristics were frequently reported, whereas evidence regarding family factors and nutritional intake or status was limited and inconsistent |
| S25 | Choi & Lee [44] (2020) | Adults with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (single-group pre–post quasi-experimental design) | Nutrition and dietary education or interventions | Following the health management education program, participants showed significant increases in overall health knowledge and all subdomain scores. Total health-promoting behavior scores also increased significantly, although changes in specific subdomains were not statistically significant |
| S26 | Cho & Park [45] (2025) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (systematic review) | Nutrition and dietary education or interventions | Common intervention techniques included high-probability request sequences, simultaneous or sequential presentation of preferred and non-preferred foods, peer modeling, and differential reinforcement. Most studies reported significant increases in food intake along with reductions in problem behaviors, although effect sizes and maintenance patterns varied by intervention setting |
| S27 | Ha & Yoo [46] (2022) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (systematic review) | Nutrition and dietary education or interventions | Gradual, repetitive, and systematic food exposure interventions for children with ASD were associated with overall improvements in food intake, food variety, food acceptance, amount consumed, and food contact behaviors. Included studies summarized clinically applicable exposure strategies and assessment tools |
| S28 | Hong & Hong [47] (2025) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Nutrition and dietary education or interventions | Most included studies focused on mental health–oriented programs for family caregivers. Interventions were associated with significant reductions in depression, anxiety, and stress, and improvements in quality of life and psychological well-being. Some studies also reported improvements in physical health behaviors such as exercise, self-care, and dietary behaviors |
| S29 | Park et al. [48] (2023) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (narrative review) | Physical activity and health promotion | Individuals with developmental disabilities demonstrated lower levels of physical activity and exercise participation than those without disabilities, along with poorer physical fitness and cardiovascular health indicators. Moderate-intensity aerobic and resistance exercise, as well as high-intensity interval training following prolonged aerobic exercise, were associated with improvements in fitness and arterial stiffness |
| S30 | Kim et al. [49] (2015) | Children and adolescents with developmental disabilities | Mixed disability groups | Observational quantitative studies (cross-sectional comparative study) | Dietary habits and nutritional status | Rates of overweight and obesity were higher in the ASD group (44%) than in the intellectual disability group (26%), and the use of appetite-stimulating medications was also more frequent in the ASD group. Functional eating difficulties such as opening beverage containers were more common in the intellectual disability group, whereas color-based food selectivity was more prevalent in the ASD group. Adolescents with intellectual disabilities consumed meat, seaweed, fats, and sugars more frequently and in larger amounts than those with ASD |
| S31 | Lee et al. [50] (2021) | Mixed (overlapping) | Mixed disability groups | Exploratory qualitative studies (focus groups and in-depth interviews; constant comparative analysis) | Nutrition and dietary education or interventions | Key themes included experiences with health problems and coping, practices of health management and education, support needs related to health management and education, and needs for school–home linked health self-advocacy programs. Teachers and parents perceived students with developmental disabilities as having physical and mental health problems, low health knowledge, and difficulties accessing healthcare services |
| S32 | Lee et al. [51] (2021) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Medical, health and clinical topics | Research topics were categorized into health status and related factors, health education and dual diagnosis issues and support, and effectiveness of exercise-centered health promotion programs. Studies were most frequently conducted in 2014, with experimental designs predominating. Most studies targeted individuals with developmental disabilities, and intervention studies primarily focused on physical activity programs |
| S33 | Cho [52] (2018) | Adults with developmental disabilities | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional SEM analysis) | Dietary habits and nutritional status | A greater number of health problems in adulthood was significantly associated with lower mental functioning and activities of daily living. Medical, community, and informal support services contributed to higher activity levels and social participation. Community services moderated the negative relationship between adult health problems and social participation |
| S34 | Whang et al. [53] (2023) | Children and adolescents with developmental disabilities | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional comparative and logistic regression analysis) | Dietary habits and nutritional status | Infants from multicultural families were significantly more likely than those from Korean families to receive abnormal results on initial developmental screening and to be diagnosed with developmental disabilities. After controlling for sex, income, and residential area, multicultural family background (foreign-born mother) remained significantly associated with developmental disability risk |
| S35 | Choi [54] (2025) | Mixed (overlapping) | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional SEM analysis) | Dietary habits and nutritional status | Family healthiness showed significant positive effects on both disability acceptance and life satisfaction. Disability acceptance was positively associated with life satisfaction and partially mediated the relationship between family healthiness and life satisfaction. Among control variables, age showed a negative association, whereas sex, disability type, education level, and presence of multiple disabilities were not significant |
| S36 | Yang et al. [55] (2019) | Mixed (overlapping) | Developmental disabilities (overall) | Intervention-based experimental studies (small-sample single-group program development and implementation) | Nutrition and dietary education or interventions | Participants demonstrated relatively high basic nutrition knowledge regarding major nutrient groups and healthy food choices. The intervention, using photo records and food models, was associated with enhanced ability to independently compose healthy meals. The program was implemented through a living-lab–based community network involving local residents, university students, and independent living support centers |
Table 3.Distribution of study types (2015–2025)
Table 4.Distribution and key characteristics of study participants
Table 5.Study types and key topic trends by disability category
Table 6.Topic-based study trend classification criteria
Table 7.Distribution and key contents by study topic (2015–2025)
Table 8.Distribution of study types by year (2015–2025)
- 1. Korean Statistical Information Service (KOSIS). Number of registered persons with disabilities by type and sex [Internet]. Ministry of Data and Statistics; 2025 [cited 2025 Dec 22]. Available from: https://kosis.kr/statHtml/statHtml.do?sso=ok&returnurl=https%3A%2F%2Fkosis.kr%3A443%2FstatHtml%2FstatHtml.do%3Fconn_path%3DMT_ZTITLE%26list_id%3DG_22%26obj_var_id%3D%26seqNo%3D%26tblId%3DDT_11761_N001%26vw_cd%3DMT_ZTITLE%26itm_id%3D%26language%3Dkor%26lang_mode%3Dko%26orgId%3D117%26
- 2. Korea Employment Agency for Persons with Disabilities. 2024 survey on work and life of persons with developmental disabilities [Internet]. Korea Employment Agency for Persons with Disabilities; 2025 [cited 2025 Dec 22]. Available from: https://www.kead.or.kr/bbs/presearch/bbsView.do?bbsCnId=206264&menuId=MENU0785
- 3. Autism Spectrum Disorder (ASD). Data and statistics on autism spectrum disorder [Internet]. ASD; 2025 [cited 2025 Dec 22]. Available from: https://www.cdc.gov/autism/data-research/index.html
- 4. Bayoumi SC, Halkett A, Miller M, Hinshaw SP. Food selectivity and eating difficulties in adults with autism and/or ADHD. Autism 2025; 29(6): 1497-1509. ArticlePubMedPMCLink
- 5. Bandini LG, Curtin C, Eliasziw M, Phillips S, Jay L, Maslin M, et al. Food selectivity in a diverse sample of young children with and without intellectual disabilities. Appetite 2019; 133: 433-440. ArticlePubMedPMC
- 6. Chistol LT, Bandini LG, Must A, Phillips S, Cermak SA, Curtin C. Sensory sensitivity and food selectivity in children with autism spectrum disorder. J Autism Dev Disord 2018; 48(2): 583-591. ArticlePubMedPMCPDF
- 7. AlFaris NA, Alshwaiyat NM, ALTamimi JZ, Alagal RI, AlSalehi SM, Al Zarah RI, et al. Nutritional status and dietary behaviors of children with intellectual or developmental disabilities in Saudi Arabia: a systematic review. J Multidiscip Healthc 2024; 17: 3371-3399. ArticlePubMedPMCLink
- 8. Bandini LG, Curtin C, Phillips SM, Rogers GT, Eliasziw M, Perelli J, et al. Nutrient adequacy, dietary patterns and diet quality among children with and without intellectual disabilities. J Intellect Disabil Res 2021; 65(10): 898-911. ArticlePubMedPMCLink
- 9. Korean Law Information Center. Act on the guarantee of rights and support for persons with developmental disabilities [Internet]. Ministry of Government Legislation; 2014 [cited 2025 Dec 24]. Available from: https://www.law.go.kr/LSW/nwRvsLsInfoR.do?lsiSeq=154060
- 10. Ministry of Health and Welfare (MOHW). 2025 guidelines for activity support services for persons with developmental disabilities [Internet]. MOHW; 2025 [cited 2025 Dec 22]. Available from: https://www.mohw.go.kr/board.es?mid=a10411010200&bid=0019&tag=&act=view&list_no=1485032
- 11. Ministry of Health and Welfare (MOHW). Announcement of the comprehensive lifelong care plan for persons with developmental disabilities [Internet]. MOHW; 2018 [cited 2025 Dec 22]. Available from: https://www.mohw.go.kr/board.es?mid=a10503010100&bid=0027&tag=&act=view&list_no=346056&cg_code
- 12. Kim JK, Lee KM, Jeon MS. Development and applicability evaluation of a nutrition education program for residents and users of disability social welfare facilities in Korea: a mixed-methods study. Korean J Community Nutr 2025; 30(1): 64-74. ArticlePubMedPMCPDF
- 13. Park JE, Kim YJ, Kim SY, Park JH. The needs and prioritization of nutrition and dietary support for individuals with disabilities: an exploratory study. Korean J Community Nutr 2024; 29(5): 431-443. ArticlePubMedPMCPDF
- 14. Individuals with Disabilities Education Act. Statute and Regulations [Internet]. U.S. Department of Education; n.d. [cited 2025 Dec 22]. Available from: https://sites.ed.gov/idea/statuteregulations/
- 15. NHS England. Joint guiding principles for integrated care systems - learning disability and autism [Internet]. NHS England; 2023 [cited 2025 Dec 22]. Available from: https://www.england.nhs.uk/publication/joint-guiding-principles-for-integrated-care-systems-learning-disability-and-autism/
- 16. National Disability Insurance Scheme (NDIS). Supports funded by the NDIS [Internet]. NDIS; 2022 [cited 2025 Dec 22]. Available from: https://www.ndis.gov.au/understanding/supports-funded-ndis
- 17. Sharp WG, Burrell TL, Jaquess DL. The autism MEAL plan: a parent-training curriculum to manage eating aversions and low intake among children with autism. Autism 2014; 18(6): 712-722. ArticlePubMedLink
- 18. Peterson KM, Piazza CC, Volkert VM. A comparison of a modified sequential oral sensory approach to an applied behavior-analytic approach in the treatment of food selectivity in children with autism spectrum disorder. J Appl Behav Anal 2016; 49(3): 485-511. ArticlePubMed
- 19. Kim YR, Kim SG, Jeon YJ. Health promotion programs for adults with developmental disabilities: a systematic review. J Korean Assoc Dev Disabil 2025; 29(2): 175-204.
- 20. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 2015; 13(3): 141-146. ArticlePubMedPMC
- 21. Kim HJ. A review of domestic research trends and future research directions on feeding behaviors and nutritional intake in individuals with developmental disabilities. J High Educ Postsec Educ Individ Disabil 2024; 3(1): 35-47. Link
- 22. Ahn MY, Moon HW, Chung HY, Park YK. Nutrient and carotenoid intakes and dietary habits in mentally disabled adults. Korean J Community Nutr 2015; 20(3): 208-219. Article
- 23. Lee SH, Hong J, Yeom JH. A qualitative inquiry on medical service improvement and support needs based on medical services and self-determination experiences of people with developmental disabilities. Korean J Phys Mult Health Disabil 2018; 61(2): 45-78. Article
- 24. Kim Y, Lee SH, Kim YR, Oh J, An H, Kim N. A qualitative inquiry into the experiences and support needs of special education teachers, nutrition teachers, and medical specialists regarding eating behaviors of students with autism spectrum disorder. J Korean Assoc Persons Autism 2021; 21(1): 57-93. Article
- 25. Lee SH, Kang HN, Kim SY. The effects health self-advocacy program with school-home connection on health care and self-determination in students with developmental disabilities. Korean J Spec Educ 2022; 57(3): 109-143. Article
- 26. Kang YS, Lee GY. The effect of a virtual reality based exercise program utilizing video game on health-related physical activity and physical activity level in adults with developmental disability. Korean J Adapt Phys Act 2015; 23(4): 15-29. Article
- 27. Lee CE, Kim KM. Research trends of mental health promotion intervention programs for families of individuals with developmental disabilities: focusing on depression. J Disabil Welf 2024; 64: 229-250. Article
- 28. Shin SY, Hwang JN, Choi SK, Heo JH. Research trends on healthcare services for individuals with developmental disabilities: a scoping review. J Spec Educ Rehabil Sci 2024; 63(3): 281-307. Article
- 29. Kim JM, Song YS. A study on the effectiveness of dietary habit improvement program for individuals with autism spectrum disorder: focused on single subjects designs. J Korean Assoc Persons Autism 2018; 18(2): 67-88. Article
- 30. Min KC, Kim BK. Understanding assessment for feeding disorders in autistic spectrum disorders: a literature review. Ther Sci Rehabil 2024; 13(2): 9-25. Article
- 31. Park HJ, Choi SJ, Kim Y, Park J, Kim YR, Lee SH, et al. Dietary behavior and food preferences according to age and the parents’ nutrition education needs of children with autism spectrum disorder. J Korean Soc Food Cult 2020; 35(3): 241-255. Article
- 32. Lee SB, Kim JY, Chung HJ, Kim SW, Im WY, Song JE. Differences of obstetric complications and clinical characteristics between autism spectrum disorder and intellectual disability. J Psychosom Med 2016; 24(2): 165-173. Article
- 33. Jeon JY, Cho BH. Applied behavioral analysis intervention effects on children with developmental disorder and swallowing disorder. Asia Pac J Multimed Serv Converg Art Humanit Sociol 2018; 8(6): 599-608. Article
- 34. Kim SY. Investigating the mediation path of eating habits on the relationship between the subjective reporting of obesity and life satisfaction. J Humanit Soc Sci 2022; 30(4): 96-118. Article
- 35. Oh TJ, Hong KS. Developmental disabilities and gut microbiota : a focus on exercise and dietary interventions. Asian J Phys Educ Sport Sci 2025; 13(3): 29-42. Link
- 36. Kim JY. Effects of exercise and nutrition education program on physical fitness and dietary habits for intellectual disabilities. Korean J Sport 2018; 16(3): 355-362. Link
- 37. Choi BY, Kang KS. The effect of music therapy applying virtual reality for the intellectually disables’ eating behavior modification. J Korean Assoc Dev Disabil 2019; 23(1): 1-19. Article
- 38. Kang SW, Kim MK. The effect of health status and challenging behavior on parents’ caregiving burden for adults with developmental disabilities. J Humanit Soc Sci 21 2020; 11(2): 17-28. Article
- 39. Kim YR, Park J, Chung SJ, An H, Kim N. Mothers’ perceptions and experiences on dietary life of their children with autism spectrum disorder. J Korean Assoc Persons Autism 2020; 20(2): 57-86. Article
- 40. Kim HY. The effect of the health education program for mothers with developmental disabled children on health care behavior and parenting stress. J Korea Acad Ind Coop Soc 2016; 17(6): 338-346. Article
- 41. Kim JK, Jeon MS. Qualitative research to build a nutrition education program operation model at social welfare facilities for people with disabilities: one-on-one in-depth interview. J Korean Diet Assoc 2024; 30(2): 83-94. Article
- 42. Ham HJ, Sohn YK. Analysis of health behavior according to life cycle and gender of people with developmental disabilities. J Korean Assoc Dev Disabil 2023; 27(4): 179-195. Link
- 43. Park J, Kim YR, Lee SH, Kim Y, Oh J, Chung SJ, et al. A literature review of eating behaviors and nutrient intake of children with autism spectrum disorders. J Korean Assoc Persons Autism 2019; 19(3): 111-132. Article
- 44. Choi A, Lee S. The effect of health care program on health knowledge and health promoting behaviors of young adults with developmental disabilities. Spec Educ Res 2020; 19(2): 101-131. Article
- 45. Cho JW, Park BR. A systematic review of ABA based interventions for eating problems in school-aged children and adolescents with ASD. J Korea Entertain Ind Assoc 2025; 19(1): 267-277. Article
- 46. Ha YN, Yoo EY. Food exposure intervention for children with autism spectrum disorders: a systematic review. J Korean Assoc Dev Disabil 2022; 26(2): 271-288. Article
- 47. Hong JW, Hong IP. Effects of intervention programs for caregivers of adults with developmental disabilities on holistic well-being: a systematic review. Korean J Occup Ther 2025; 33(1): 25-39. Article
- 48. Park W, Lee JS, Kim SH, Lee JS, Kim HJ, Sung S, et al. A literature review study on physical fitness and cardiovascular health in people with developmental disabilities and exercise. Asian J Phys Educ Sport Sci 2023; 11(5): 119-130. Link
- 49. Kim Y, Son JH, Lim Y. Eating habits and dietary intakes of Korean adolescents with intellectual disabilities and autism spectrum disorders. J Korean Soc Wellness 2015; 10(3): 265-275. Link
- 50. Lee SH, An H, Choi J, Kim A, Yang J. A qualitative inquiry on experiences and support needs of special education teachers and parents regarding health care and education for students with developmental disabilities. J Yeolin Educ 2021; 29(6): 129-158. Article
- 51. Lee S, An H, Jung J, Kim GH. Review of research trends and future research directions regarding the health of people with developmental disabilities. Spec Educ Res 2021; 20(2): 31-61. Article
- 52. Cho SE. The association of health and multidimensional disability by the types of support systems among adults with developmental disabilities: using the international classification of functioning, disability and health (ICF). Korean J Health Educ Promot 2018; 35(2): 49-59. Article
- 53. Whang W, Lee SJ, Rho YS, Nam EW. A comparative study on infant development disability: Korean and multi-cultural families. Korean Public Health Res 2023; 49(2): 67-77. Article
- 54. Choi JE. The effect of family strength on life satisfaction among individuals with developmental disabilities: the mediating role of disability acceptance. J Korean Assoc Dev Disabil 2025; 29(2): 225-240. Link
- 55. Yang KM, Cheon YJ, Kim BC, Yoon WJ, Kim SJ, Lee JS, et al. Development of a healthy dietary education program for independent dietary practice among adults with developmental disabilities. Proceedings of The 4TH Industrial Revolution: The Role of Fodd & Nutritional Sciences; 2019 Oct 23-25; Jeju: p. 376. Link
- 56. Ptomey LT, Wittenbrook W. Position of the academy of nutrition and dietetics: nutrition services for individuals with intellectual and developmental disabilities and special health care needs. J Acad Nutr Diet 2015; 115(4): 593-608. ArticlePubMed
- 57. Dean S, Marshall J, Whelan E, Watson J, Zorbas C, Cameron AJ. A systematic review of health promotion programs to improve nutrition for people with intellectual disability. Curr Nutr Rep 2021; 10(4): 255-266. ArticlePubMedPDF
- 58. Santos FH, Zurek J, Janicki MP. Efficacy of healthy aging interventions for adults with intellectual and developmental disabilities: a systematic review. Gerontologist 2022; 62(4): e235-e252. ArticlePubMedPMCPDF
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteResearch trends in dietary behaviors and nutrition education among individuals with developmental disabilities in Korea: a scoping review (2015–2025)
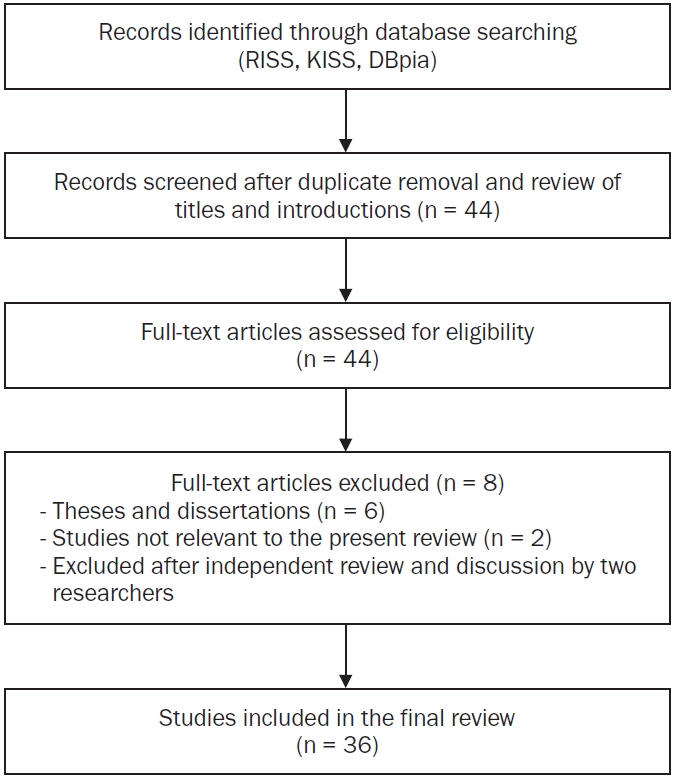
Fig. 1. Flow diagram of the literature selection process (adapted from the Joanna Briggs Institute scoping review methodology).
Fig. 1.
Research trends in dietary behaviors and nutrition education among individuals with developmental disabilities in Korea: a scoping review (2015–2025)
| Category | Content |
|---|---|
| Databases | RISS, KISS, DBpia |
| Search period | January 2015–September 2025 |
| Population-related keywords | developmental disabilities, intellectual disability, autism spectrum disorder |
| Diet and nutrition-related keywords | dietary habits, nutrition, nutritional status, diet, dietary patterns, intake, eating behavior, food preference, obesity, chronic diseases, weight management, health promotion |
| Nutrition education and intervention-related keywords | nutrition education programs, nutrition intervention, caregiver perception |
| Search strategy | Population-related keywords were combined with diet and nutrition or nutrition education and intervention-related keywords using the AND operator |
| Example search formula | (developmental disabilities OR intellectual disability OR autism spectrum disorder) AND (dietary habits OR nutritional status OR dietary patterns OR health promotion) |
| Study ID | Reference | Population | Disability type | Study design | Main topic | Key findings |
|---|---|---|---|---|---|---|
| S1 | Kim et al. [19] (2025) | Adults with developmental disabilities | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Physical activity and health promotion | Included studies primarily targeted adults with mild to moderate intellectual disabilities and most frequently used single-group pre–post designs. Interventions reported overall positive changes in anthropometric measures, physical fitness, physical activity levels, dietary behaviors, health knowledge, self-efficacy, and quality of life. Few studies assessed maintenance/generalization, intervention fidelity, or social validity. Programs mainly focused on nutrition education, physical activity information, and exercise participation, frequently using visual supports and reinforcement strategies |
| S2 | Kim [21] (2024) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Dietary habits and nutritional status | Domestic studies have increased since 2012, with most employing literature reviews or survey designs. Qualitative and intervention studies were relatively scarce, and study populations were concentrated on children and individuals with multiple disabilities. Common dietary behavior issues included food selectivity, texture sensitivity, fear of new foods, pica, and atypical eating patterns |
| S3 | Ahn et al. [22] (2015) | Adults with developmental disabilities | Mixed disability groups | Observational quantitative studies (cross-sectional survey) | Dietary habits and nutritional status | Mean BMI indicated overweight in the intellectual disability group and obesity in the mental disability group. Intake frequencies of vegetables and dairy products were generally low. Both groups showed vitamin B1, B2, and calcium intakes below recommended levels. Carotenoid intake, particularly lycopene, was lower than that of the general population, and cryptoxanthin intake was also low in the mental disability group |
| S4 | Lee et al. [23] (2018) | Mixed (overlapping) | Developmental disabilities (overall) | Exploratory qualitative studies (in-depth interviews and focus groups; constant comparative analysis) | Medical, health and clinical topics | Key findings included difficulties in expressing and recognizing illness and symptoms, practical challenges in health management, barriers in access and communication during medical encounters, and limited self-determination in healthcare. Individuals with developmental disabilities experienced restricted access to information and decision-making due to communication difficulties and reliance on caregivers, with lack of disability awareness, inadequate facilities, and financial burden identified as major barriers |
| S5 | Kim et al. [24] (2021) | Professionals and teachers | Autism spectrum disorder | Exploratory qualitative studies (in-depth interviews and focus groups; constant comparative analysis) | Dietary habits and nutritional status | Major themes included types of eating behaviors, eating-related problems, influencing factors (individual, environmental, medical), coping and instructional strategies, instructional difficulties, and support needs. Common eating behavior problems among students with ASD included food selectivity, texture sensitivity, food refusal, and pica, with gastrointestinal symptoms, sensory and behavioral characteristics, and home–school environments interacting to influence eating behaviors |
| S6 | Lee et al. [25] (2022) | Children and adolescents with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (single-group pre–post) | Nutrition and dietary education or interventions | Following the health education intervention, students’ health knowledge and health-promoting behavior scores significantly increased compared with baseline. Ninety-three percent of participants achieved health management goals at or above the expected level. Self-determination significantly increased in student self-ratings, whereas no significant changes were observed in parent or teacher ratings |
| S7 | Kang & Lee [26] (2015) | Adults with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (randomized controlled pre–post design) | Physical activity and health promotion | Muscle mass increased most in the APA + Wii group, whereas body fat mass decreased most in the APA group. Muscular endurance, strength, flexibility, and cardiorespiratory fitness improved more in groups including APA than in the Wii-only group, while balance improved most in the Wii group. Step counts and caloric expenditure increased in all intervention groups compared with controls |
| S8 | Lee & Kim [27] (2024) | Parents and caregivers | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Medical, health and clinical topics | Depression intervention programs for families of individuals with developmental disabilities showed overall significant reductions in depressive symptoms. Most programs were short-term (fewer than 10 sessions) group-based interventions, with reported effect sizes in the moderate to large range |
| S9 | Shin et al. [28] (2024) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (scoping review) | Medical, health and clinical topics | Regular health checkups were identified as the most highly needed healthcare service. Across the life course, early diagnosis and early intervention were prioritized in infancy, whereas prevention of early aging and medical support were emphasized in middle and older adulthood. Individuals with developmental disabilities exhibited higher prevalence of chronic diseases, increased risk of premature mortality, and lower access to healthcare services, indicating substantial health vulnerability |
| S10 | Kim & Song [29] (2018) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (meta-analysis) | Nutrition and dietary education or interventions | The overall intervention effect size was Tau-U = 0.876, indicating moderate to high effectiveness. Larger effects were observed at younger ages and during follow-up phases compared with intervention phases. Multicomponent interventions were more effective than single-technique approaches, with the greatest effects reported for interventions lasting less than 20 sessions and approximately 2 months (5–8 weeks) |
| S11 | Min & Kim [30] (2024) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (narrative review) | Dietary habits and nutritional status | Feeding disorders in children with ASD were reported to be highly diverse, highlighting the need for comprehensive assessment. Available assessment tools were limited, and the inclusion of additional domains such as oral-motor and digestive function was recommended |
| S12 | Park et al. [31] (2020) | Mixed (overlapping) | Autism spectrum disorder | Observational quantitative studies (cross-sectional survey) | Dietary habits and nutritional status | BMI distribution differed by age, with higher rates of underweight among children aged ≤ 10 years and higher rates of overweight and obesity among adolescents aged 11–19 years. Most participants consumed snacks at least once daily. Food preferences differed across age groups for grains, vegetables, fruits, dairy products, fats, and sugars. Parents reported high needs and willingness to participate in nutrition education |
| S13 | Lee et al. [32] (2016) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Observational quantitative studies (retrospective medical record review) | Medical, health and clinical topics | At the first visit, children with ASD had a higher proportion of males, fewer obstetric complications, and lower receptive and expressive language scores than children with intellectual disabilities. Children whose diagnosis changed from intellectual disability to ASD were all male, had more frequent family histories of developmental delay, and showed significantly lower initial receptive language scores. Sex, language characteristics, and obstetric information were associated with early ASD identification |
| S14 | Jeon & Cho [33] (2018) | Children and adolescents with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (single-case design) | Medical, health and clinical topics | After intervention, meal intake increased to approximately 700–800 g, with reductions in frequent small meals and shorter mealtime duration. Feeding patterns shifted from predominantly formula-based intake (≥ 80%) to mixed feeding after one week and to 100% solid food intake after two weeks. Applied behavior analysis intervention was associated with reductions in food refusal behaviors |
| S15 | Kim [34] (2022) | Adults with developmental disabilities | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional survey with mediated regression analysis) | Dietary habits and nutritional status | Higher levels of perceived obesity were associated with poorer dietary habits and lower life satisfaction. Regular meals and balanced nutrition were positively correlated with both dietary habit scores and life satisfaction. Dietary habits showed a significant mediating effect in the relationship between perceived obesity and life satisfaction |
| S16 | Oh & Hong [35] (2025) | Adults with developmental disabilities | Developmental disabilities (overall) | Evidence synthesis studies (narrative review) | Medical, health and clinical topics | Individuals with developmental disabilities showed reduced gut microbiota diversity, increased harmful bacteria, and decreased beneficial bacteria, which were associated with neurotransmitter dysregulation, immune and inflammatory responses, and metabolic imbalance. Dietary modification, probiotic supplementation, and physical activity interventions were reported to improve gut microbiota balance and related metabolic pathways |
| S17 | Kim [36] (2018) | Adults with developmental disabilities | Intellectual disability | Evidence synthesis studies (single-group pre–post) | Physical activity and health promotion | After 16 weeks of intervention, no significant changes were observed in body composition indicators (BMI, body fat percentage). However, flexibility, muscular strength, and power significantly improved. Dietary habit scores increased, with higher intake frequencies of protein, green-yellow vegetables, and seaweed, and reduced intake of salty foods, sweets, and late-night snacks |
| S18 | Choi & Kang [37] (2019) | Adults with developmental disabilities | Intellectual disability | Intervention-based experimental studies (multiple-baseline single-subject design) | Physical activity and health promotion | All participants showed increased numbers of appropriate eating behaviors during intervention and maintenance phases compared with baseline. Mean performance increased from 3.2 of 13 behaviors at baseline to 7 during intervention and 11 during maintenance. VR-based social story music therapy was associated with improvements in eating behavior performance and social skill acquisition |
| S19 | Kang & Kim [38] (2020) | Parents and caregivers | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional survey with hierarchical multiple regression) | Dietary habits and nutritional status | Poorer health status and higher levels of challenging behaviors in adults with developmental disabilities were significantly associated with increased caregiver burden. Health status and challenging behaviors were identified as significant predictors of caregiver burden |
| S20 | Kim et al. [39] (2020) | Parents and caregivers | Autism spectrum disorder | Exploratory qualitative studies (thematic analysis of in-depth interviews) | Dietary habits and nutritional status | Mothers’ experiences were categorized into themes related to children’s eating characteristics (clear food preferences, atypical eating behaviors, influence of past experiences), family interactions, efforts to improve dietary behaviors, and support needs. Children’s eating behavior problems imposed burdens on family meals, dining out, and mealtime atmosphere, with coping strategies involving environmental modification, consistent guidance, and program participation |
| S21 | Kim [40] (2016) | Parents and caregivers | Developmental disabilities (overall) | Intervention-based experimental studies (non-equivalent control group pre–post–follow-up design) | Nutrition and dietary education or interventions | Compared with the control group, the intervention group showed significantly greater improvements in children’s health management behaviors over time. Parenting stress scores in the intervention group significantly decreased at post-test and follow-up, with larger reductions than those observed in the control group |
| S22 | Kim & Jeon [41] (2024) | Professionals and teachers | Developmental disabilities (overall) | Exploratory qualitative studies (one-on-one in-depth interviews) | Nutrition and dietary education or interventions | The most frequently requested nutrition education topics were diet education for obesity prevention and management and basic nutrition knowledge. Education at kindergarten to lower elementary school level was considered appropriate given cognitive functioning. Activity-based, face-to-face education using real foods, cooking activities, and visual materials, delivered in sessions of approximately 30 minutes, was perceived as effective |
| S23 | Ham & Sohn [42] (2023) | Mixed (overlapping) | Developmental disabilities (overall) | Observational quantitative studies (secondary data analysis with two-way ANOVA) | Dietary habits and nutritional status | Smoking, alcohol consumption, and stress showed significant main effects across both life stage and sex. Overweight showed a significant main effect by life stage, whereas sexual health issues differed by sex. Significant interaction effects between life stage and sex were observed for all five health behaviors, with higher levels reported for specific subgroups such as adolescent males’ sexual health issues and older adults’ alcohol use or overweight |
| S24 | Park et al. [43] (2019) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (narrative review) | Dietary habits and nutritional status | Many studies reported that children with ASD exhibited atypical eating behaviors such as food selectivity, binge eating, and pica compared with typically developing children. Data collection relied mainly on parent reports and observations. Associations between eating behaviors and individual characteristics were frequently reported, whereas evidence regarding family factors and nutritional intake or status was limited and inconsistent |
| S25 | Choi & Lee [44] (2020) | Adults with developmental disabilities | Developmental disabilities (overall) | Intervention-based experimental studies (single-group pre–post quasi-experimental design) | Nutrition and dietary education or interventions | Following the health management education program, participants showed significant increases in overall health knowledge and all subdomain scores. Total health-promoting behavior scores also increased significantly, although changes in specific subdomains were not statistically significant |
| S26 | Cho & Park [45] (2025) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (systematic review) | Nutrition and dietary education or interventions | Common intervention techniques included high-probability request sequences, simultaneous or sequential presentation of preferred and non-preferred foods, peer modeling, and differential reinforcement. Most studies reported significant increases in food intake along with reductions in problem behaviors, although effect sizes and maintenance patterns varied by intervention setting |
| S27 | Ha & Yoo [46] (2022) | Children and adolescents with developmental disabilities | Autism spectrum disorder | Evidence synthesis studies (systematic review) | Nutrition and dietary education or interventions | Gradual, repetitive, and systematic food exposure interventions for children with ASD were associated with overall improvements in food intake, food variety, food acceptance, amount consumed, and food contact behaviors. Included studies summarized clinically applicable exposure strategies and assessment tools |
| S28 | Hong & Hong [47] (2025) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Nutrition and dietary education or interventions | Most included studies focused on mental health–oriented programs for family caregivers. Interventions were associated with significant reductions in depression, anxiety, and stress, and improvements in quality of life and psychological well-being. Some studies also reported improvements in physical health behaviors such as exercise, self-care, and dietary behaviors |
| S29 | Park et al. [48] (2023) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (narrative review) | Physical activity and health promotion | Individuals with developmental disabilities demonstrated lower levels of physical activity and exercise participation than those without disabilities, along with poorer physical fitness and cardiovascular health indicators. Moderate-intensity aerobic and resistance exercise, as well as high-intensity interval training following prolonged aerobic exercise, were associated with improvements in fitness and arterial stiffness |
| S30 | Kim et al. [49] (2015) | Children and adolescents with developmental disabilities | Mixed disability groups | Observational quantitative studies (cross-sectional comparative study) | Dietary habits and nutritional status | Rates of overweight and obesity were higher in the ASD group (44%) than in the intellectual disability group (26%), and the use of appetite-stimulating medications was also more frequent in the ASD group. Functional eating difficulties such as opening beverage containers were more common in the intellectual disability group, whereas color-based food selectivity was more prevalent in the ASD group. Adolescents with intellectual disabilities consumed meat, seaweed, fats, and sugars more frequently and in larger amounts than those with ASD |
| S31 | Lee et al. [50] (2021) | Mixed (overlapping) | Mixed disability groups | Exploratory qualitative studies (focus groups and in-depth interviews; constant comparative analysis) | Nutrition and dietary education or interventions | Key themes included experiences with health problems and coping, practices of health management and education, support needs related to health management and education, and needs for school–home linked health self-advocacy programs. Teachers and parents perceived students with developmental disabilities as having physical and mental health problems, low health knowledge, and difficulties accessing healthcare services |
| S32 | Lee et al. [51] (2021) | Mixed (overlapping) | Developmental disabilities (overall) | Evidence synthesis studies (systematic review) | Medical, health and clinical topics | Research topics were categorized into health status and related factors, health education and dual diagnosis issues and support, and effectiveness of exercise-centered health promotion programs. Studies were most frequently conducted in 2014, with experimental designs predominating. Most studies targeted individuals with developmental disabilities, and intervention studies primarily focused on physical activity programs |
| S33 | Cho [52] (2018) | Adults with developmental disabilities | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional SEM analysis) | Dietary habits and nutritional status | A greater number of health problems in adulthood was significantly associated with lower mental functioning and activities of daily living. Medical, community, and informal support services contributed to higher activity levels and social participation. Community services moderated the negative relationship between adult health problems and social participation |
| S34 | Whang et al. [53] (2023) | Children and adolescents with developmental disabilities | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional comparative and logistic regression analysis) | Dietary habits and nutritional status | Infants from multicultural families were significantly more likely than those from Korean families to receive abnormal results on initial developmental screening and to be diagnosed with developmental disabilities. After controlling for sex, income, and residential area, multicultural family background (foreign-born mother) remained significantly associated with developmental disability risk |
| S35 | Choi [54] (2025) | Mixed (overlapping) | Developmental disabilities (overall) | Observational quantitative studies (cross-sectional SEM analysis) | Dietary habits and nutritional status | Family healthiness showed significant positive effects on both disability acceptance and life satisfaction. Disability acceptance was positively associated with life satisfaction and partially mediated the relationship between family healthiness and life satisfaction. Among control variables, age showed a negative association, whereas sex, disability type, education level, and presence of multiple disabilities were not significant |
| S36 | Yang et al. [55] (2019) | Mixed (overlapping) | Developmental disabilities (overall) | Intervention-based experimental studies (small-sample single-group program development and implementation) | Nutrition and dietary education or interventions | Participants demonstrated relatively high basic nutrition knowledge regarding major nutrient groups and healthy food choices. The intervention, using photo records and food models, was associated with enhanced ability to independently compose healthy meals. The program was implemented through a living-lab–based community network involving local residents, university students, and independent living support centers |
| Research type | Number (n) | Percentage (%) | Key characteristics |
|---|---|---|---|
| Observational quantitative studies | 10 | 27.8 | Assessment of dietary habits, nutrient intake, obesity status, and nutritional imbalances based on cross-sectional or comparative data |
| Exploratory qualitative studies | 5 | 13.9 | In-depth exploration of dietary experiences, self-determination, and perceived support needs of individuals with developmental disabilities and caregivers |
| Intervention-based experimental studies | 8 | 22.2 | Education-, exercise-, and behavior-based short-term participatory programs evaluating changes in health behaviors and dietary outcomes |
| Evidence synthesis studies | 13 | 36.1 | Systematic reviews, scoping reviews, and meta-analyses synthesizing intervention effects, research trends, and policy or service accessibility |
| Total | 36 | 100.0 |
| Research subject | Number (n) | Main study types | Key characteristics | Research focus |
|---|---|---|---|---|
| Children and adolescents | 10 | Observational quantitative, intervention-based experimental, evidence synthesis | Multidimensional approaches addressing feeding problems and sensory sensitivity | School- and family-based dietary education and interventions integrating sensory and emotional factors |
| Adults | 9 | Intervention-based experimental, observational quantitative, evidence synthesis | Integrated approaches combining exercise and nutrition education | Development of behavior-change–focused and context-sensitive intervention models |
| Parents and caregivers | 4 | Observational quantitative, intervention-based experimental, evidence synthesis | Care burden, parenting stress, and parent-focused education | Family-based health promotion and nutrition education programs |
| Professionals and teachers | 2 | Exploratory qualitative | Exploration of field experiences and educational needs | Practice-based insights and needs for multidisciplinary collaboration |
| Mixed or multiple groups | 11 | Observational quantitative, exploratory qualitative, evidence synthesis | Collaborative approaches involving parents, teachers, and professionals | Expansion of coordinated and integrated nutrition and health education models |
| Disability category | Number of studies [n (%)] | Composition of study types | Main research topics | Summary of findings |
|---|---|---|---|---|
| Developmental disabilities (overall) | 22 (61.1) | Observational quantitative (6), intervention-based experimental (6), exploratory qualitative (2), evidence synthesis (8) | Eating behaviors and nutrient intake; health management and health promotion programs; obesity, physical activity, and quality of life; caregiver health education; dysphagia, gut microbiota, and healthcare services | Studies addressed a wide range of health-related topics, with intervention studies focusing on health behaviors and quality of life outcomes |
| Autism spectrum disorder | 8 (22.2) | Exploratory qualitative (2), observational quantitative (1), evidence synthesis (5) | Sensory sensitivity; food refusal; feeding guidance; experiences of parents and teachers; age-related eating behaviors and food preferences; exposure-based and applied behavior analysis-informed feeding approaches | Research primarily focused on feeding-related problems and behavioral characteristics |
| Intellectual disability | 2 (5.6) | Intervention-based experimental (2) | Exercise and nutrition education programs; virtual reality- or music-based interventions | Limited number of intervention studies addressing physical fitness and lifestyle-related outcomes |
| Mixed disability groups | 4 (11.1) | Observational quantitative (3), exploratory qualitative (1) | Health management and educational experiences of students with disabilities; dietary intake patterns; obstetric complications; nutrient and carotenoid intake | Studies examined diverse health and nutrition issues across heterogeneous disability groups |
| Category | Examples of subtopics | Corresponding research methods |
|---|---|---|
| Dietary habits and nutritional status | Dietary patterns, food frequency, nutrient intake, obesity and weight status, eating behaviors, meal attitudes | Observational quantitative studies; qualitative studies (exploration of caregiver, student, or professional perspectives); evidence synthesis studies (review of dietary and nutritional status) |
| Nutrition and dietary education or interventions | Nutrition education programs, dietary behavior interventions, feeding interventions, family- and teacher-involved programs | Intervention-based experimental studies; quasi-experimental designs; qualitative studies (program implementation and participation experiences); evidence synthesis studies (systematic or narrative reviews of interventions) |
| Physical activity and health promotion | Exercise interventions, physical fitness, cardiovascular health, physical activity levels, obesity prevention, health management behaviors | Intervention-based experimental studies (exercise-based or combined approaches); evidence synthesis studies (reviews of physical activity and health promotion programs) |
| Medical, physiological, and clinical topics | Gut microbiota, feeding disorders, nutritional metabolism, physiological indicators, health screening, disease-related factors, healthcare access | Clinical and observational studies; comparative studies; qualitative studies (healthcare experiences); evidence synthesis studies (scoping or systematic reviews of medical and healthcare topics) |
| Research topic category | Number of studies (n) | Main study populations | Predominant study types | Examples of subtopics | Summary of research focus |
|---|---|---|---|---|---|
| Dietary habits and nutritional status | 14 | Children/adolescents, adults | Primarily observational quantitative; some qualitative | Dietary patterns, food frequency, nutrient intake, obesity and weight status, eating behaviors, meal attitudes | Studies examined imbalances in nutrient intake (e.g., calcium and B vitamins), selective eating, and obesity patterns, as well as caregiver and professional perspectives on dietary practices |
| Nutrition and dietary education or interventions | 10 | Adults, children, parents, teachers | Predominantly intervention-based; some qualitative and evidence synthesis | Nutrition education, dietary behavior interventions, feeding interventions, family- and teacher-involved programs | Research focused on changes in dietary behaviors, self-determination, meal-related attitudes, and caregiver practices following educational or behavioral interventions |
| Physical activity and health promotion | 5 | Mainly adults | Predominantly intervention-based; some evidence synthesis | Exercise interventions, physical fitness, cardiovascular health, physical activity levels, obesity prevention, health management behaviors | Studies investigated physical health outcomes, body composition, and fitness improvements associated with structured physical activity or combined intervention programs |
| Medical, physiological, and clinical topics | 7 | Adults, children, older adult women with developmental disabilities | Clinical, observational, and evidence synthesis | Gut microbiota, dysphagia, nutritional metabolism, physiological indicators, health screening, healthcare access | Research explored medical and physiological characteristics, feeding and swallowing disorders, and healthcare access issues related to nutrition and health among individuals with developmental disabilities |
| Research type | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | 2025 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention-based experimental studies | 1 | 1 | 2 | 2 | 1 | 1 | 8 | |||||
| Exploratory qualitative studies | 1 | 1 | 1 | 1 | 1 | 5 | ||||||
| Observational quantitative studies | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 10 | ||||
| Evidence synthesis studies | 1 | 1 | 1 | 1 | 1 | 4 | 4 | 13 | ||||
| Total | 3 | 2 | 0 | 5 | 3 | 4 | 2 | 4 | 3 | 5 | 5 | 36 |
Table 1. Literature search strategy and keyword combinations
Table 2. Characteristics of included studies
BMI, body mass index; ASD, autism spectrum disorder; APA, adapted physical activity; VR, virtual reality; ANOVA, analysis of variance.
Table 3. Distribution of study types (2015–2025)
Table 4. Distribution and key characteristics of study participants
Table 5. Study types and key topic trends by disability category
Table 6. Topic-based study trend classification criteria
Table 7. Distribution and key contents by study topic (2015–2025)
Table 8. Distribution of study types by year (2015–2025)
n.


